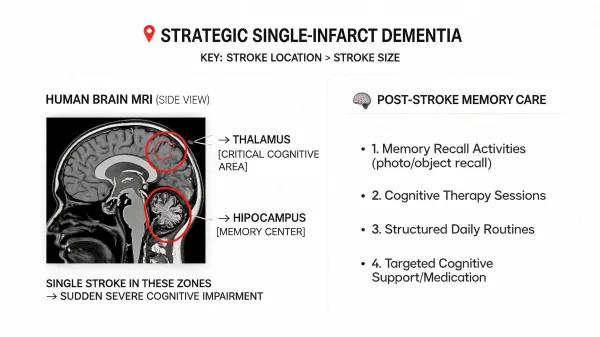
Strategic single-infarct dementia is a form of vascular dementia caused by a single stroke in a critical brain region, such as the thalamus, hippocampus, or angular gyrus, where even a small area of damage can produce severe and lasting cognitive impairment.
If your parent was independent last week and today can't remember your name after what the doctor called a "small stroke," you're not imagining things and you're not overreacting. Some strokes hit areas of the brain where even a tiny amount of damage changes everything. The medical team may have used the word "minor," but what you're witnessing at home tells a completely different story.
Most people associate strokes with physical symptoms: weakness on one side, slurred speech, difficulty walking. But some strokes cause damage you can't see from the outside. When a stroke hits certain regions of the brain, the physical effects may be minimal while the cognitive effects are devastating. Your parent might walk and talk and look the same, but they can't form new memories, can't follow a conversation, or can't recognize people they've known for decades. The disconnect between how they look and how they function is what makes this so confusing for families trying to understand what happened.
Unlike multi-infarct dementia, which develops gradually after repeated small strokes over time, strategic single-infarct dementia results from one event, one stroke, and a sudden, permanent shift in your parent's cognitive ability. When our family went through a sudden cognitive decline with a loved one, the hardest part wasn't the diagnosis itself. It was the speed. One day everything was normal, and the next day it wasn't. That kind of whiplash is something no amount of reading can fully prepare you for, but understanding what happened inside the brain can help you make sense of what you're seeing now and give you a foundation for the care decisions ahead.
This article explains why the location of a stroke matters far more than its size, what strategic brain areas are most vulnerable, and what the care path looks like when one stroke changes everything.
Why One Small Stroke Can Cause Major Cognitive Damage
Families are often told the stroke was "small" or "minor," and they expect a full recovery. When that recovery doesn't come, the confusion is overwhelming. The reason is that stroke severity is measured primarily by size and by physical deficits. A stroke that doesn't cause paralysis or impair speech production and doesn't show up as a large lesion on imaging gets classified as minor. But that classification doesn't account for where the stroke occurred, and in the brain, location determines the outcome far more than size.
Strategic Brain Areas and Why They Matter
Certain regions of the brain serve as critical relay hubs for cognition, memory, and behavior. These areas are physically small, but they sit at the intersection of neural networks that control how we think, remember, learn, and make decisions. When a stroke destroys tissue in one of these regions, the damage ripples outward through entire networks, producing cognitive deficits far out of proportion to the size of the lesion. Neurologists refer to these as "strategic" locations because a single infarct there can produce widespread cognitive disruption that would normally require multiple strokes in less critical areas.
The thalamus acts as the brain's central switchboard, routing sensory information, regulating attention, and connecting to nearly every region of the cerebral cortex. It plays a direct role in memory formation, executive function, and personality. Research has found that thalamic infarction carries nearly a fivefold increase in the risk of cognitive decline within 12 months, regardless of how physically minor the event appeared. Even a unilateral thalamic stroke can disrupt the thalamo-cortical circuits enough to cause lasting problems with memory, attention, and the ability to plan or organize daily tasks.
The hippocampus is the brain's primary center for forming new memories. When a stroke destroys hippocampal tissue, the result is often sudden and severe anterograde amnesia, meaning your parent loses the ability to create new memories from the moment of the stroke forward. They may recall events from 20 years ago with clarity but can't remember what happened five minutes ago. I've seen situations in the hospital where the initial scan didn't catch everything, and it took further imaging to reveal what was actually going on. That delay can leave families in limbo, wondering why their parent seems so different when the tests seem normal.
The angular gyrus sits at the junction of the parietal and temporal lobes and serves as an integration hub for language, memory, spatial awareness, and sensory processing. A stroke here can produce deficits that closely resemble Alzheimer's disease: difficulty reading, writing, and understanding language, combined with spatial disorientation and trouble retrieving autobiographical memories.
Understanding What the Neurologist Is Telling You
When the neurologist explains the imaging results, you may hear terms like "lacunar infarct" or "focal ischemic event," both of which describe a relatively small area of brain tissue that lost blood supply and died. The key question isn't "how big was the stroke?" It's "where was the stroke?" If the answer involves the thalamus, hippocampus, angular gyrus, caudate nucleus, or capsular genu, you're dealing with a strategic infarct, and the cognitive consequences may be permanent regardless of how small the lesion appears on the scan.
What Strategic Single-Infarct Dementia Looks Like Day to Day
The daily reality depends heavily on which brain area was affected, and each type of strategic stroke produces a distinct pattern of deficits that families learn to recognize over time. A thalamic stroke may leave your parent struggling with attention, planning, and initiative, sitting passively for hours without starting or completing tasks they used to handle automatically. A hippocampal stroke often means your parent repeats the same questions every few minutes, can't remember meals they just ate, and doesn't retain new information regardless of how many times it's explained. An angular gyrus stroke can make reading, writing, and even recognizing familiar objects or places difficult, sometimes to a degree that resembles advanced Alzheimer's even when the stroke happened only weeks earlier.
What makes this particularly hard for families is that the physical person often looks unchanged. Your parent can walk, feed themselves, smile and greet you at the door. But the cognitive architecture behind daily functioning has been fundamentally altered, and that contrast between physical appearance and cognitive reality is one of the most disorienting aspects of this condition. It's why well-meaning friends and relatives often don't understand the severity of the situation when they visit. They see your parent laughing at a joke or pouring a cup of coffee and assume things are fine. They don't see the same question asked twelve times in an hour or the look of total confusion when something breaks from the routine. Having worked in hospitals for nearly 20 years, I've seen how easily that gap between appearance and reality can mislead even experienced clinicians, let alone family members who are seeing the person for the first time since the stroke. The visible isn't the whole story, and the people closest to your parent are usually the first to notice what others miss.
When the Medical Language Doesn't Match What You're Seeing
In practice, this is where things break down for families. The ER or hospital team may document a "minor stroke" because the physical deficits are minimal. Insurance coding may classify the event as low-severity based on those same physical metrics. Discharge paperwork might recommend outpatient follow-up with no particular urgency. Meanwhile, you're watching your parent ask the same question for the tenth time in an hour, and no one in the medical system seems alarmed by what you're describing.
This disconnect isn't malicious, but it is dangerous. Stroke severity scales were designed to measure physical impairment, not cognitive impact. The National Institutes of Health Stroke Scale, the standard tool used in emergency settings, weights motor function and speech production heavily but doesn't capture the kind of memory, reasoning, and behavioral deficits that strategic infarcts produce. A parent who scores low on that scale can still have profound dementia. If what you're observing at home doesn't match the "minor" label in the medical chart, trust what you're seeing. Push for neuropsychological testing, request a referral to a neurologist who specializes in vascular cognitive impairment, and document the specific changes you've noticed with dates and examples. That documentation becomes critical for both medical care and eventual care planning.
When Memory Care Becomes the Right Step
Not every strategic single-infarct dementia case requires immediate memory care placement. Some families manage for months or even years at home with the right combination of in-home support, family involvement, and environmental modifications like removing stove knobs, installing door alarms, and simplifying the layout of the home so your parent can move through it without becoming disoriented. But the decision point usually arrives when safety becomes a daily concern rather than an occasional worry. If your parent is wandering outside the home, leaving appliances on, unable to manage medications independently, or becoming agitated in ways that put them or others at risk, a structured care environment with trained staff may be the safest option available. Consider a situation where your parent gets up at 3 a.m., unlocks the front door, and walks down the street in their pajamas, confused about where they are. That's the kind of event that shifts the conversation from "we can manage at home" to "we need help we can't provide."
The sudden onset of strategic single-infarct dementia often compresses the timeline families expect for these decisions. With Alzheimer's disease, there's typically a gradual decline that gives families months or years to research options and plan financially. With a strategic stroke, the need for memory care can arise within weeks of the event. I've watched families go from "everything is fine" to researching care facilities in a matter of days, and there's no gentle way through that transition. Knowing this compressed timeline is a real possibility can help you start gathering information before the decision becomes urgent.
What Memory Care Offers After a Strategic Stroke
Memory care communities are designed for residents living with dementia, regardless of the underlying cause. For someone with strategic single-infarct dementia, the features that matter most include 24-hour supervised environments designed to prevent wandering, structured daily routines that reduce confusion and anxiety, staff trained specifically in redirecting agitation and managing behavioral changes, and medication management for secondary conditions like post-stroke depression or seizure prevention.
One thing worth communicating clearly to the memory care team is that your parent's condition resulted from a vascular event, not a progressive neurodegenerative disease like Alzheimer's. This distinction matters for care planning because the cognitive profile may differ significantly from a typical Alzheimer's resident. Some cognitive functions, particularly long-term memory and certain practical skills, may remain largely intact even while short-term memory or language abilities are severely impaired. A care team that understands this can tailor activities and daily routines to what your parent can still do, preserving dignity and engagement in ways that a one-size-fits-all dementia approach might miss. Ask the facility how they adapt care plans for residents with vascular dementia specifically, and pay attention to whether the staff seems familiar with the difference. That conversation alone will tell you a lot about the quality of the program.
Costs and Financial Planning for Memory Care
Memory care costs in 2025 range from roughly $5,000 to over $10,000 per month depending on location, level of care, and the specific community. National median estimates from the CareScout 2025 Cost of Care Survey put assisted living at around $6,200 per month, with memory care typically running 20% to 30% higher due to the specialized staffing and security these communities require. At the midrange, that's roughly $7,500 to $8,000 monthly, or $90,000 to $96,000 per year. For a two-to-three-year stay, families should plan for $180,000 to $290,000 or more, and those numbers can climb considerably in higher-cost regions.
When our family first saw the real numbers for memory care, it felt like being hit twice: first the diagnosis, then the cost. Most families haven't budgeted for this kind of expense because most families never imagined a single stroke could create this level of need this quickly. Medicare doesn't cover memory care residential costs. Medicaid may help if your parent qualifies financially, but eligibility rules and waitlists vary significantly by state. Long-term care insurance, VA Aid and Attendance benefits for qualifying veterans, and personal savings or home equity are the most common funding sources families turn to. Start the financial conversation early, even while you're still adjusting to the diagnosis, because the options narrow quickly once placement becomes urgent.
Finding Your Way Through the Hardest Part
Strategic single-infarct dementia rewrites the rules families thought they understood about strokes. A "small" stroke in the wrong location can permanently change your parent's cognitive ability, and the speed of that change is something most families are completely unprepared for. Understanding that this is a recognized medical condition with specific neurological explanations, not something you're imagining or exaggerating, is the first step toward getting your parent the right care.
Ask the neurologist where the stroke occurred and what cognitive functions that region controls. Push for comprehensive neuropsychological testing that documents the specific deficits, because that documentation will shape everything from care planning to financial assistance applications. And give yourself permission to grieve the sudden loss of the parent you knew yesterday, even while they're still standing in front of you. You didn't cause this, and you can't reverse it. But you can make sure your parent is safe, supported, and cared for in a way that respects who they still are. That's not a small thing.