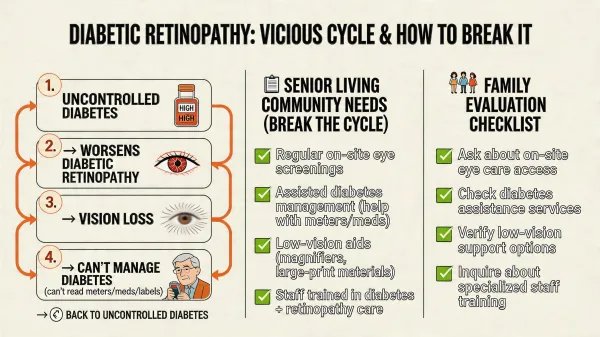
When diabetes takes your parent's vision, it also takes away their ability to manage the very disease that's blinding them. That's the cruel math of diabetic retinopathy in a senior living context. The tiny blood vessels in the retina get damaged by years of blood sugar fluctuations, and as those vessels break down, so does your parent's ability to read a glucose meter, draw up insulin accurately, or see the subtle changes on their feet that signal an infection. Every task that keeps diabetes in check depends on vision your parent is losing.
Here's what makes diabetic retinopathy different from other senior living conversations: it isn't just a vision problem. It's a self-reinforcing loop where poor vision leads to medication errors, medication errors lead to worse blood sugar control, and worse blood sugar control accelerates the retinopathy. By the time most families see what's happening, the A1C has been climbing for months, and the eye disease has already progressed to a stage where treatment can only slow the damage, not reverse it.
This article walks through how diabetic retinopathy interacts with diabetes self-management, what a senior living community needs to provide to break that cycle, how to evaluate whether a community can handle both conditions at once, and how families can tell when home care has stopped working. The goal isn't to pressure anyone toward a specific decision. It's to give you enough specific information to recognize where your parent actually is on this continuum and what kind of support the situation really calls for.
What Diabetic Retinopathy Means for Senior Living Decisions
Diabetic retinopathy is damage to the blood vessels in the retina caused by chronically high blood sugar. It's the leading cause of vision loss in adults with diabetes, progressing through four recognized stages from mild nonproliferative retinopathy to proliferative retinopathy with fragile new vessels that can bleed into the eye. Diabetic macular edema, swelling in the central part of the retina, can happen at any stage and is the most common cause of actual vision loss.
About one in three adults over 40 with diabetes already shows signs of diabetic retinopathy, per the National Eye Institute, and roughly 29% of Americans over 65 have diabetes. What matters for senior living isn't the eye damage itself but what it breaks. Diabetes self-management is one of the most vision-dependent chronic disease regimens in medicine, and once reliable vision goes, every piece of the regimen starts to fail at once.
The Vicious Cycle: Vision Loss Makes Diabetes Harder, Diabetes Makes Vision Worse
The compounding problem works in both directions, which is what makes diabetic retinopathy uniquely dangerous among the conditions that push families toward senior living.
How Poor Glucose Control Accelerates Retinal Damage
Sustained hyperglycemia is the main driver of diabetic retinopathy progression. High glucose weakens the walls of the retinal capillaries, causes microaneurysms, triggers inflammatory changes, and leads to capillary closure and the release of growth factors that prompt abnormal blood vessel growth. Strict glucose control, per the NIH, is the single most effective way to slow retinopathy. The early stages are partially reversible if blood sugar comes down and stays down, but the later stages can't be reversed.
The implication is direct. A parent whose blood sugar swings between 60 and 400 because they can't accurately dose insulin is accelerating their own blindness with every mis-measured dose. The median time from moderate nonproliferative retinopathy to severe or proliferative retinopathy is roughly two years, per NIH data, and a year of uncontrolled glucose during that window can shift a parent from a favorable prognosis to a conversation about preventing total blindness.
The Diabetes Tasks That Require Adequate Vision
Most families underestimate how vision-dependent diabetes really is. Every day your parent has to read the number on a glucose meter, see the small lines on an insulin syringe or the dial on a pen, distinguish long-acting from rapid-acting insulin on medication labels, count carbohydrates from nutrition labels in tiny print, inspect their feet for cuts or blisters that signal a diabetic ulcer, and read pharmacy instructions after every medication change.
Any single task can be worked around with the right tools. Talking meters exist, insulin pens have audible clicks, and magnifiers help with labels. Working around all of them at once, without help, while the parent also has age-related memory changes and arthritic fingers, is where the system breaks. A 2023 study on diabetes device accessibility found that most insulin pens and glucose monitors lack meaningful accessibility features for people with vision loss, and patients who can't find reliable assistance frequently end up administering doses incorrectly.
The Downward Spiral Families Don't See Coming
Here's how the spiral plays out. Your parent's vision starts slipping, but they don't mention it, either because they don't want to worry you or because the changes have been gradual enough that they've adjusted without noticing. They start guessing at insulin doses, usually erring low because a little too low feels safer than a little too high. Blood sugar creeps up, higher glucose accelerates the retinal damage, vision worsens, and the dose guessing becomes even less accurate. They have a hypoglycemic episode because they misread the dial and injected twice the units they meant to. A few months later, their A1C is 10.2, their macular edema has progressed, and you're in a senior living conversation that wasn't on anyone's radar six months ago. In my hospital work, I've seen variations of this land in the ER repeatedly, and the gap between what families believed was happening at home and what was actually happening is almost always wider than anyone expected.
Breaking the Cycle: What a Care Community Must Provide
The only thing that reliably breaks the spiral is structural, external oversight of the vision accommodations and the diabetes regimen together, every day. Most communities can do parts of this, but fewer can do all of it, and knowing what to look for is how you tell the difference.
Supervised Insulin Administration
This is the most important capability and the most variable across communities. State regulations differ on who can administer insulin: some states allow trained medication aides, while others restrict it to licensed nurses. That means the community needs an LPN or RN on-site during medication rounds, a contracted home health nurse, or it can't safely take your parent at all. Before you tour, get a direct answer on who administers the dose, how many times per day, and what happens on weekends and overnight. The distinction most families miss is between medication reminders (handing your parent an insulin pen and saying "time for your shot") and medication administration (a trained staff member confirms the insulin type, measures the dose, and gives the injection), and your parent needs the latter.
Large-Display Monitors, Voice-Enabled Devices, and Low-Vision Accommodations
A well-equipped community should pair diabetes care with low-vision tools rather than treat them as separate problems. That means talking glucose meters like the Prodigy Voice or EmbraceTALK, continuous glucose monitors with smartphone integration that family or staff can monitor remotely, insulin pens with audible click-per-unit dosing, large-print medication charts, contrast-enhanced lighting, and tactile markers on door handles. Ask the community to walk you through exactly what devices they use with current low-vision diabetic residents. If they can't name specific equipment, they don't have a system.
Evaluation Criteria That Separate Good Communities from Good Marketing
Use these questions during tours to cut through the brochure language:
- Can your nursing staff administer insulin, and how many times per day?
- What happens if my parent has a hypoglycemic episode at 3 a.m.?
- How do you coordinate with an ophthalmologist for recurring anti-VEGF injection appointments, which are typically monthly for the first several doses and then roughly every 8 weeks?
- Do you have experience with residents who need both low-vision accommodations and active insulin management, and can I speak to the nurse who oversees that care?
- What's your protocol when a resident's A1C trends upward over consecutive months?
The answers you want are specific, not reassuring: "we work closely with all our residents' doctors" is marketing, but "our director of nursing faxes A1C results and insulin logs to the endocrinologist every 90 days, or sooner if there's a change" is a system.
Where Things Actually Break Down at Home
In practice, this is where things break down. A parent insists they can still manage their diabetes, and they've done it for 20 years, so they don't want help, and they especially don't want to move, and the family agrees to give it another few months. Meanwhile, the insulin doses are off, sometimes by a unit or two and sometimes by ten, and nobody knows because the parent doesn't log anything they can't clearly see. By the time the family catches it, usually after the parent passes out in the kitchen or shows up confused at a holiday dinner, the A1C has spiked into the double digits and the next eye exam shows the retinopathy has moved from moderate to severe. The hard part isn't the decision. It's the timing. Families who move earlier, before the crisis, generally preserve more vision and better overall diabetes control than families who wait.
A Realistic Picture: When Guessing at Doses Becomes the Norm
Consider a situation where your father has diabetic retinopathy that's been progressing for two years. He can still see well enough to get around his house, and he swears he can still read his glucose meter. What he hasn't told you is that he can only read it if he holds it four inches from his face in bright sunlight, and he can't reliably tell a 7 from a 1 on the insulin syringe markings. He's been guessing at doses for six months, giving himself too little on some days (and running 280) and too much on others (catching himself feeling shaky before he eats a handful of crackers).
His A1C has climbed from 7.1 to 9.4 in a year, and his ophthalmologist noted at the last visit that the retinopathy progressed from moderate nonproliferative to severe nonproliferative. The endocrinologist keeps adjusting the regimen, but adjustments only work if they're followed exactly, and exactly is no longer possible at home. The regimen isn't the problem. The ability to execute the regimen is, and that's the pattern behind a large percentage of older adults with diabetic retinopathy living alone.
What I've Seen Inside the Facilities
During the years I did mobile X-ray work inside rest homes and skilled nursing facilities, I spent a lot of time in medication rooms and resident rooms, usually positioning patients for chest films or hip X-rays. One pattern in the lower-quality facilities has stuck with me: diabetic residents struggled with medication management because nobody on staff had ever assessed whether they could read the labels on their own prescription bottles, insulin vials sat next to other clear vials with no tactile markings, and residents squinted at glucose meters they couldn't see. Every one of those residents had a chart listing "diabetes" and "vision impairment" as separate problems, managed separately, as if the two had nothing to do with each other. Nobody was connecting the dots, and that disconnected approach to care is exactly what the right community should never look like.
What a Good Care Community Looks Like in Practice
When the vision accommodations and diabetes management actually work together, the difference shows within weeks. Blood sugar stabilizes because doses are correct and consistent, and the parent eats balanced meals at regular times, which is a massive part of glucose control and one of the things communities genuinely do well. Foot checks happen on a schedule because nursing staff rolls them into the daily routine, and small problems get caught before they turn into ulcers. Ophthalmology appointments happen on time because transportation is coordinated rather than left to the parent, and for those receiving ongoing intravitreal anti-VEGF injections for diabetic macular edema, this coordination alone can save vision. Missing injections, or starting and stopping the schedule because transportation fell through, is associated with worse visual outcomes.
Cost Considerations for Vision-Impaired Diabetic Care
Diabetes-specific care in senior living usually sits at the higher end of the assisted living price range. As of 2025, the national median monthly cost for assisted living is roughly $5,900, though figures vary by region and level of care. A community that administers insulin multiple times per day, coordinates low-vision accommodations, and manages complex medication schedules often adds $500 to $1,500 per month in care-level fees, or $7,000 to $18,000 annually on top of the roughly $71,000 base. That adds up fast.
For families weighing in-home care against a community, the raw monthly number can look comparable until you factor in what diabetic retinopathy actually requires. An in-home caregiver who administers insulin four times a day, handles foot checks, coordinates eye injections, and monitors blood sugar overnight typically runs 10 to 12 hours a day at $30 to $40 an hour, totaling $9,000 to $15,000 per month for partial coverage. Round-the-clock home care, which a late-stage retinopathy patient on insulin realistically needs, can exceed $20,000 per month, and most families don't plan for this. Medicare doesn't pay for long-term custodial care, Medicaid may cover some costs in qualifying facilities for residents who meet income and asset limits (rules vary by state), and long-term care insurance often covers a portion when activities-of-daily-living triggers are met.
Deciding What Level of Care Diabetic Retinopathy Actually Requires
Not every older adult with diabetic retinopathy needs assisted living. The right level depends on how advanced the retinopathy is, how complex the diabetes regimen is, and what other conditions are in the mix.
A parent with mild nonproliferative retinopathy, stable A1C under 8.0, oral medications only (no insulin), and no other significant cognitive or functional issues can often stay home safely with periodic check-ins, a talking glucose meter, and pharmacy-level medication packaging. A parent with moderate to severe retinopathy, insulin-dependent diabetes, A1C trending upward, and any hypoglycemia in the past year is at high risk of the spiral described earlier. This parent needs active daily oversight, and if family can't provide it, assisted living with diabetes-specific nursing is the right match. A parent with proliferative retinopathy, frequent insulin adjustments, active macular edema requiring regular anti-VEGF injections, or a recent diabetes-related hospitalization is no longer a good candidate for home care except under narrow circumstances. Assisted living with enhanced diabetes care, or a skilled nursing facility if the medical complexity is high, is the appropriate level.
Questions Families Commonly Ask
Can my parent keep seeing their current ophthalmologist after moving to a community?
Usually yes, if the community is within a reasonable drive, and most communities coordinate outside specialist appointments and provide transportation. Confirm during the tour how they handle recurring appointments like anti-VEGF injections, which can't be postponed without risking vision loss.
What if my parent refuses to go to a community?
This is common and rarely has a clean answer, but what sometimes works is framing the move around a specific benefit your parent cares about (reliable meals, social connection, relief from household responsibilities) rather than the medical reasoning. Many communities offer short-term respite stays that let a parent try the environment without committing, and when refusal is rooted in fear, a tour with the specific nurse who would manage their diabetes often helps more than any brochure.
How fast can diabetic retinopathy actually progress?
Faster than most families expect. With poor glucose control, moderate nonproliferative retinopathy can advance to severe or proliferative stages within roughly two years, per published NIH data, and diabetic macular edema can cause noticeable vision loss within months. Early treatment with anti-VEGF injections and laser therapy when indicated can slow or stop progression, but it can't reverse existing damage.
Does Medicare cover anti-VEGF injections?
Medicare Part B typically covers medically necessary anti-VEGF injections for diabetic macular edema and proliferative diabetic retinopathy, though patients are generally responsible for the Part B deductible and 20% coinsurance unless they have supplemental coverage. Coverage specifics can change, so verify with Medicare.gov or the ophthalmologist's billing office before starting a new regimen.
Where to Go From Here
Diabetic retinopathy isn't just a vision problem, and it isn't just a diabetes problem. It's a compounding problem that gets worse on its own unless something external breaks the cycle. The right senior living community can do that by pairing insulin administration with low-vision accommodations, coordinating eye care appointments, and catching the slow drift in A1C before it becomes a crisis. Families who act earlier tend to preserve more of their parent's vision and more of their parent's independence, counterintuitive as that sounds.
Start with an honest assessment of where your parent is on the stages of retinopathy, how consistent their diabetes management has actually been (not what they say, what the numbers show), and what's realistically sustainable at home. From there, the decision usually becomes clearer than it looked at the start. You don't have to figure this out all at once. The next right step is often a conversation with your parent's endocrinologist, a call to the ophthalmologist's office to understand the stage, or a first tour of a community that specializes in diabetic care. The goal isn't to move faster than your family is ready for, it's to stop letting the cycle decide for you.