This article describes emerging diagnostic technologies and is intended for informational purposes only. It isn't medical advice and doesn't replace consultation with your parent's healthcare provider. Insurance coverage of these tools varies, and laws governing how predictive test results can be used by insurers and employers continue to evolve. Talk with your family's physician and, where appropriate, an attorney or financial advisor before making decisions based on early-detection results.
As of April 2026, AI dementia detection has moved from research papers into the clinic. Tools published in peer-reviewed journals over the past eighteen months can analyze a single brain scan, a routine eye exam, or a few minutes of recorded speech and flag patterns associated with Alzheimer's disease and other dementias years before traditional diagnosis would be possible.
In Main Radiology for most of my career, I've watched AI quietly change what medical imaging can find. A decade ago, radiologists were the only ones reading the scan. Now algorithms flag findings, prioritize cases, and catch subtleties that pattern-trained eyes sometimes miss. Dementia diagnosis is going through that same shift right now, and the implications for families are bigger than most people realize.
Years of earlier warning is both a gift and a weight. It's a gift because earlier knowledge means earlier planning, earlier conversations, and a longer window to make decisions while your parent can still participate in them. It's a weight because earlier knowledge can also mean years of anxiety without a proven treatment, and predictive results that aren't fully protected from insurance discrimination.
This piece walks through the real AI tools detecting dementia years before symptoms appear, what's clinically available right now versus what's still in research, and what families should think about before pursuing predictive testing. If your parent is already showing early signs of dementia, this is a useful companion to the standard evaluation pathway.
Can AI Detect Dementia Years Before Symptoms?
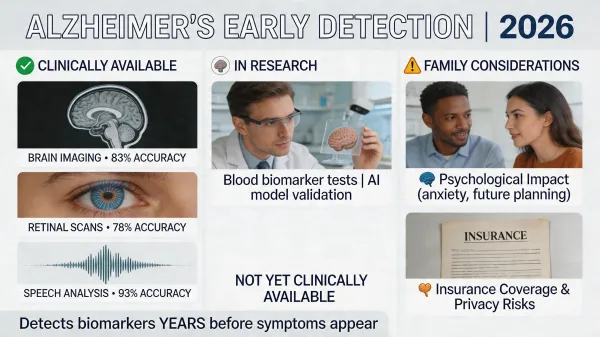
Yes. As of 2026, AI tools can identify Alzheimer's and related dementias years before clinical symptoms appear. Brain imaging analysis, retinal scans, and speech pattern analysis show real-world accuracy ranging from 78% to 93% depending on the method, with the strongest speech-based research predicting cognitive decline up to six years before traditional diagnosis.
The Mayo StateViewer Tool and What It Can Do
The most clinically advanced AI dementia detection tool right now is Mayo Clinic's StateViewer, published in Neurology in June 2025. StateViewer analyzes a single FDG-PET scan, a type of brain imaging that shows how cells in different regions of the brain are using glucose, and identifies which of nine specific types of dementia the patient is most likely to have. The list includes Alzheimer's disease, Lewy body dementia, frontotemporal dementia, and several rarer forms.
The peer-reviewed accuracy figure is 88%. The tool was trained on more than 3,600 scans from patients with confirmed diagnoses, and Mayo's research team reports it produces results nearly twice as fast as standard interpretation workflows and up to three times more accurate at distinguishing between dementia subtypes. That distinction matters because Alzheimer's, Lewy body, and frontotemporal dementias respond differently to medications and require different care planning.
From a radiology workflow standpoint, FDG-PET scans aren't new. The technology has been used in oncology and neurology for years. What's changed is having a tool that can read those scans with subtype-level precision and produce a confidence-ranked report a neurologist can use to guide diagnosis. In a busy clinic, this kind of decision support shaves hours off the interpretation timeline and gives families a clearer answer faster.
StateViewer is currently deployed at Mayo Clinic affiliated sites and is expected to spread through 2026 and 2027 as Mayo's licensing partnerships extend the tool to additional health systems. If your parent is being evaluated for dementia at a major academic medical center, it's reasonable to ask whether StateViewer or a similar AI-assisted PET interpretation tool is part of the workup. At a smaller community hospital or local neurology practice, it probably isn't yet. That gap will close, but it'll close on a timeline of years, not months.
One practical note on cost and coverage: Medicare covers FDG-PET for diagnostic differentiation between Alzheimer's and frontotemporal dementia in patients meeting clinical criteria, and most major commercial insurers follow Medicare's lead. The scan itself runs several thousand dollars. AI-assisted interpretation typically doesn't add cost to the patient because it sits inside the radiology workflow rather than as a separately billable service. The barrier is access to centers using the technology, not the financial structure of the scan itself.
AI Dementia Detection Through Retinal Scans
The second major frontier is the eye. The retina shares developmental origin with brain tissue, which is why ophthalmologists have long called it "the window to the brain." Researchers have spent the past several years building AI models that can detect signs of cognitive decline by analyzing retinal images, and the results have been strong enough to attract major industry attention.
The most prominent tool right now is Eye-AD, a deep learning framework highlighted by NVIDIA in 2025 for its work analyzing optical coherence tomography angiography, a non-invasive scan that maps the tiny blood vessels at the back of the eye. In published research, Eye-AD reached 93.55% accuracy detecting early-onset Alzheimer's disease from these images. The scan itself takes minutes, doesn't require dye injection, and is similar in patient experience to a standard eye exam at an optometry clinic. Separately, researchers at the National University of Singapore published work on a tool called RetiPhenoAge that estimates a person's "retinal age" from a standard fundus photograph and compares it to their chronological age. People whose retinal age was significantly higher than their actual age showed 25% to 40% higher risk of cognitive decline over time. This is research-stage work, but it points to a future where annual eye exams could include cognitive risk screening as a routine output for adults over a certain age.
The strongest argument for retinal AI dementia detection is access. Eye exams are common, relatively inexpensive, covered by Medicare and most insurance plans, and don't require specialty referrals. If retinal AI tools clear regulatory review and reach optometry chains, screening could happen during a normal vision check at no marginal cost to the patient. That's a different economic model than PET imaging, which requires nuclear medicine equipment, specialty staff, and several thousand dollars per scan.
For now, retinal AI dementia detection remains primarily research. A few specialty memory clinics offer it as part of broader cognitive risk panels, but it isn't routinely available through community optometrists. Expect that to change over the next two to three years.
Speech Pattern Analysis Years Before Diagnosis
The most striking AI dementia research published in the past two years comes from speech pattern analysis. NIA-funded research released in 2024 showed that machine learning models analyzing how someone talks, not what they say, can predict Alzheimer's disease with 78.2% accuracy up to six years before clinical diagnosis. Other multi-modal research from MIT-affiliated teams has produced comparable findings.
The signals the AI is reading aren't dramatic. They're subtle changes in vocabulary diversity, sentence complexity, the length and frequency of pauses, the time spent searching for a word, and the substitution of general words ("thing," "stuff") for specific ones. These shifts begin years before a family would notice anything wrong. They're invisible to the speaker. They're invisible to most listeners. The AI sees them in patterns built from thousands of recorded interviews.
The practical implication is that this kind of testing could eventually happen at a primary care visit. A patient reads a paragraph, describes a picture, or has a five-minute conversation while a microphone records. The audio is analyzed, and a risk score appears in the medical chart along with blood pressure and weight. No imaging. No needle. No specialist referral. That's a fundamentally different screening pipeline than what we have now.
Watching a family member's dementia accelerate, in retrospect, the speech changes were the earliest signal. Word-finding pauses we wrote off as normal aging. A vocabulary that quietly narrowed before her short-term memory began to slip. Sentences that lost their old precision. None of us recognized those patterns in real time, and even if we had, no doctor in 2018 would have done anything about them. An AI screen at her annual checkup three or four years before diagnosis would have given the family an entirely different planning window. Whether we would have wanted that information sooner is a question I still think about.
Several consumer-facing apps and digital cognitive assessments are already incorporating speech analysis features, though FDA-cleared and clinically validated tools remain limited. Expect speech-based screening to be the most rapidly democratized of the three AI dementia detection methods, because it requires only a phone or laptop microphone and no specialty equipment.
The Psychological and Insurance Weight of Earlier Detection
Earlier detection ahead of effective treatment is the central tension of AI dementia detection. The drugs that exist right now, lecanemab and donanemab, slow disease progression modestly in early Alzheimer's. They aren't cures, they require infusions, they carry real side effect risk, and they're approved for specific patient profiles. For most people identified as high-risk by an AI tool today, no current treatment is going to reverse the trajectory.
That creates years of knowing without a clear path to action. The psychological weight of that is real. Some patients want to know early so they can put legal and financial documents in place, have hard conversations while their parent is still themselves, and plan for care funding before the financial pressure hits. Others would rather not carry that knowledge for half a decade with nothing they can do about it. Both responses are reasonable.
The insurance picture is more concerning. The Genetic Information Nondiscrimination Act, passed in 2008, protects against discrimination based on genetic test results in health insurance and employment. It doesn't cover amyloid biomarker tests, AI-based predictive tests, or most of the new generation of pre-symptomatic dementia indicators. It also doesn't cover long-term care insurance, life insurance, or disability insurance at all. What that means in practice is that if your parent or you receive an AI-based positive risk score for Alzheimer's, applying for long-term care insurance afterward is likely to result in denial or significantly higher premiums. The same applies to life insurance. The same applies to individual disability insurance. Some states have additional protections, but federal coverage of predictive cognitive testing barely exists right now. Anyone considering pursuing these tests proactively should talk to a financial advisor or elder law attorney about insurance sequencing before testing, not after.
From inside hospitals, I've watched patients carry years of anxiety from inconclusive findings on imaging studies, sometimes findings that turned out to mean nothing at all. The psychological cost of carrying a high-risk dementia signal for half a decade isn't theoretical. It's a real thing families need to weigh carefully before pursuing predictive testing, and it's a conversation that should happen before the test, not after the result.
What Families Can Access Right Now
The clinical reality of AI dementia detection in April 2026 breaks down by tool.
Mayo StateViewer is clinically deployed at Mayo Clinic sites and starting to roll out to partner health systems. If your parent's evaluation is happening at a Mayo location or a major academic neurology center, it's reasonable to ask whether AI-assisted PET interpretation is being used in the workup. At community hospitals and most independent neurology practices, it isn't available yet.
Eye-AD and retinal AI dementia detection tools are primarily research-stage. A handful of specialty memory clinics include retinal scanning in their cognitive risk panels, but routine availability through community optometrists is at least two years out.
Speech pattern analysis is the most fragmented. The clinically validated tools sit inside research clinics and digital health pilots. Several consumer apps offer speech-based cognitive checks, but their accuracy and clinical validity vary widely. Treat consumer apps as flagging tools at best, not diagnostic ones.
Blood tests for Alzheimer's biomarkers, separately, are commercially available and can be ordered through a regular physician's office. They're a different category of early detection than the AI tools described here, but for families looking for accessible early signals today, blood-based testing is the most reachable option.
The practical move for any family considering AI-assisted dementia evaluation is to call your parent's neurologist and ask what's available at their institution. The answer varies enormously by location, and a Mayo or Cleveland Clinic referral may put a substantially different toolkit on the table than a local community practice.
How AI Dementia Detection Is Changing the Primary Care Visit
The most plausible near-term shift is in primary care, not specialty clinics. Within one to three years, routine screening combining a five-minute speech check, a retinal scan during the annual eye exam, and a blood biomarker panel for adults over sixty becomes a realistic standard of care. None of those individual pieces requires technology that doesn't already exist. The integration is the work in progress, along with the FDA clearance pathways and reimbursement codes that have to follow.
That's a different healthcare system than the one we have now. It moves dementia from a condition diagnosed reactively after symptoms surface to a condition screened for proactively before symptoms exist. The clinical, ethical, and financial implications of that transition are still being worked out by professional societies, payers, and federal regulators, and families who are paying attention now will be in a better position when those changes arrive.
The Bottom Line for Families
AI dementia detection is real, it's accelerating, and it's reshaping what doctors can know about cognitive risk years before symptoms emerge. For families evaluating a parent who's already showing signs, the most important question to ask is what AI-assisted tools are available at the institution doing the evaluation. For families thinking about long-term planning, the most important conversation is about insurance sequencing before any predictive testing happens, and about understanding the full cost of memory care in case earlier signals lead to earlier planning.
The technology will keep moving fast. The medical system, insurance protections, and legal frameworks will move slower. Your job isn't to chase every announcement. It's to know what's available, ask informed questions, and make decisions that fit your family's specific situation. The earlier you start that conversation, the better.