When Your Parent Stops Eating Because It Hurts
Your father pushes his plate away after two bites. He doesn't say anything, but you can see it in his face. The pain that's coming is worse than the hunger he's sitting with right now. He's made this calculation before, probably dozens of times this week alone, and hunger keeps losing.
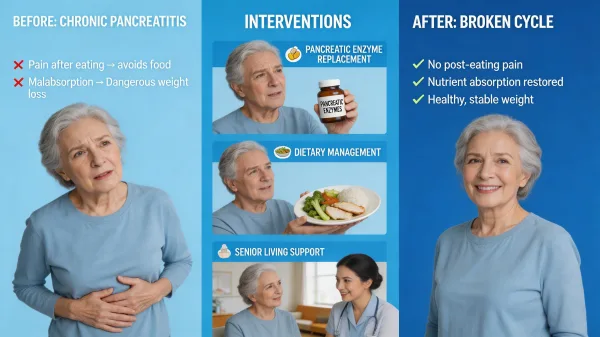
This is what chronic pancreatitis looks like from across the dinner table. It's not a dramatic emergency. It's a quiet, grinding condition where the pancreas stays inflamed, digestion slowly fails, and the simple act of eating becomes something your parent dreads. Over weeks and months, the weight drops. The clothes get looser. The energy fades. And the person you're watching isn't refusing food out of stubbornness or depression. They're avoiding it because their body has taught them that eating means suffering.
For families trying to manage chronic pancreatitis care at home, the daily demands can feel relentless. Your parent needs to eat small, carefully prepared low-fat meals throughout the day. They need pancreatic enzyme supplements timed precisely with each meal and snack. They need pain managed on a schedule that accounts for the fact that pain spikes after eating. And they need someone watching their weight, their nutrition, and their hydration closely enough to catch a downward slide before it becomes a crisis. When that level of daily support exceeds what family caregivers can realistically provide, chronic pancreatitis senior living options deserve serious consideration.
I spent years as a caregiver for someone whose relationship with food became defined by pain. Watching a person you love associate eating with suffering changes how you think about mealtime forever. That experience is part of why I feel strongly that families dealing with chronic pancreatitis deserve honest information about what daily care actually requires and when a structured environment might offer something home care can't.
Understanding Chronic Pancreatitis in Older Adults
Chronic pancreatitis is a progressive inflammatory condition where the pancreas sustains irreversible damage over time. Unlike acute pancreatitis, which flares and resolves, the chronic form causes ongoing fibrosis and scarring that gradually destroys the organ's ability to produce digestive enzymes and regulate blood sugar. The condition affects roughly 50 out of every 100,000 people in the United States, with incidence and prevalence both increasing with age. Approximately one third of all pancreatitis patients are aged 65 or older.
In older adults, the causes shift somewhat. While alcohol use remains the most common cause overall (responsible for roughly 40% to 70% of cases depending on the study), seniors are more likely to develop chronic pancreatitis from gallstone-related damage, medication effects, or causes that are never clearly identified. The condition is also harder to diagnose in older patients because symptoms can overlap with other gastrointestinal problems, and imaging findings in aging pancreases can mimic early chronic pancreatitis even without true disease. Abdominal pain is the most common symptom, affecting roughly 75% of patients at diagnosis, and this pain worsens as the disease progresses.
What matters most for families isn't the cause. It's understanding that chronic pancreatitis doesn't get better. The damage is cumulative. Management focuses on controlling pain, replacing lost digestive function, and preventing malnutrition, all of which require consistent daily attention.
Why Eating Becomes the Enemy
The cruelest part of chronic pancreatitis is the trap it sets around food. When you eat, your pancreas tries to produce digestive enzymes. In a damaged pancreas, this effort triggers inflammation, pressure buildup in blocked or narrowed ducts, and nerve irritation that produces severe epigastric pain, often radiating to the back. The pain typically starts within 30 minutes of eating and can last for hours.
Your parent learns this pattern fast. The body connects eating with pain, and a powerful avoidance response takes hold. They skip meals. They eat less at each sitting. They gravitate toward bland, minimal food that barely sustains them. Families often describe watching their parent shrink, losing 20 or 30 pounds over a few months while insisting they're "just not hungry."
But they are hungry. The problem isn't appetite. The problem is that their body punishes them for eating. Without intervention, this cycle accelerates. Less food means less nutrition. Less nutrition means muscle wasting, weakened immunity, fatigue, and cognitive changes. Each of those makes the person less capable of managing their own care, which makes the cycle harder to break.
Pain vs. Nutrition: The Daily Balancing Act of Chronic Pancreatitis
What most people don't realize until they're in it is that chronic pancreatitis care isn't really about one big medical decision. It's about dozens of small daily decisions around food, enzymes, pain, and timing that have to be made correctly, consistently, every single day. Miss the enzymes at one meal and your parent pays for it with hours of pain and diarrhea. Eat too much fat and the same thing happens. Skip a meal to avoid the pain and malnutrition creeps forward another step. This is the daily balancing act that defines life with this condition.
Pancreatic enzyme replacement therapy, often called PERT, is the cornerstone of managing malabsorption from chronic pancreatitis. These prescription medications (brand names include Creon, Zenpep, and Pancreaze) contain lipase, protease, and amylase extracted from porcine pancreas. They replace the enzymes your parent's pancreas can no longer produce in adequate amounts. Research confirms that PERT significantly improves fat absorption, reduces steatorrhea (the oily, foul-smelling stools characteristic of malabsorption), and helps stabilize body weight in patients with exocrine pancreatic insufficiency. The timing is critical: enzymes must be taken with the first bite of food and sometimes spread across the meal if eating takes longer than 15 to 20 minutes. They need to be swallowed with cold or room-temperature liquids because heat deactivates them. Getting the dose right requires working with a gastroenterologist, because the amount of lipase units varies based on the fat content of each meal, the severity of the insufficiency, and individual response.
Dietary management works alongside enzyme therapy. Current guidelines recommend that patients with chronic pancreatitis eat a well-balanced diet with adequate protein, keeping total fat intake around 30 to 50 grams per day spread across four to six small meals rather than three large ones. Fat is the key trigger. The more fat in a meal, the harder the pancreas works, and the more likely pain will follow. Medium-chain triglycerides (MCTs), found in coconut oil and available as supplements, can provide additional calories because they're absorbed differently and don't require the same pancreatic enzyme activity. Patients also need monitoring for deficiencies in fat-soluble vitamins (A, D, E, and K) and micronutrients like B12, zinc, and folic acid, since malabsorption doesn't just affect calories.
Alcohol abstinence is non-negotiable. Alcohol decreases lipase activity, makes PERT less effective, accelerates pancreatic damage, and directly increases pain. Even small amounts can trigger flares. For seniors with a history of alcohol use, this requirement adds another layer of monitoring and support that families need to plan for.
I've watched a loved one go through the cruel arithmetic of needing food to survive while knowing that eating will bring pain. It changes how you understand what "mealtime support" actually means. It's not just cooking and serving. It's timing enzymes correctly, preparing foods that fall within strict fat limits, offering encouragement when your parent would rather skip the meal entirely, and monitoring whether what they're eating is actually being absorbed. When our family went through this with a loved one's illness, I saw how quickly mealtimes can shift from normal routine to a source of dread for everyone at the table. A structured care environment where trained staff manage enzyme timing, prepare appropriate meals, and track nutritional intake daily can break the avoidance cycle in ways that family caregivers, despite their best efforts, often can't sustain around the clock.
Signs Your Parent May Need More Support Than Home Can Provide
There's no single moment when home care stops being enough. It's usually a pattern. Consider the scenario where your parent has lost 30 pounds over several months because the abdominal pain after meals is so severe that they've all but stopped eating full meals. They're malnourished but caught between two impossible choices: eat and suffer, or avoid food and decline. A structured care environment can step into that gap with consistent enzyme management, pain protocols, and meals designed around their specific restrictions.
Watch for these patterns: unintentional weight loss that continues despite your efforts, enzyme doses being missed or taken incorrectly, pain that keeps your parent from eating even when food is prepared for them, repeated ER visits for pain crises or dehydration, and your own exhaustion as a caregiver trying to manage a complex medical regimen alongside everything else in your life. Any one of these is worth a conversation with your parent's gastroenterologist about whether a senior living community with appropriate medical support might offer better daily outcomes.
What Chronic Pancreatitis Care Looks Like in Senior Living
Not every assisted living community is equipped to handle the daily complexity of chronic pancreatitis. The communities that do it well share certain characteristics. Their dining programs can accommodate medically restricted diets, including low-fat meal preparation with accurate nutritional tracking. Their medication management systems can handle enzyme timing (with the first bite of food, not on a generic medication schedule). Their staff understand that a resident who pushes food away isn't being difficult. They're in pain.
Good communities also coordinate with outside specialists. Your parent will still need a gastroenterologist managing their overall treatment plan, and the community should be able to communicate changes in weight, appetite, pain frequency, and stool patterns back to that physician. Some communities offer on-site dietitian services, which is a significant advantage for residents with complex nutritional needs. Having someone who understands the difference between "low-fat" and "appropriate fat for exocrine insufficiency" matters more than it sounds.
From my years working inside the healthcare system, I've seen how much gets lost between a doctor's care plan and what actually happens day to day. A good care environment closes that gap.
Finding the Right Community for Complex Digestive Conditions
When touring communities, ask specific questions. Can the kitchen prepare meals within a prescribed fat gram limit per meal? How does staff handle enzyme administration timing (with meals, not from a medication cart that arrives at a set time)? What happens when a resident is in too much pain to eat? Is there a protocol for tracking weight and nutritional intake, and how often is that data reviewed?
Ask about pain management philosophy too. Chronic pancreatitis pain requires a multimodal approach, often combining non-opioid analgesics, neuromodulators like pregabalin, and careful use of stronger medications when needed. Communities that default to "call the doctor if there's a problem" without having standing pain management protocols may not be the right fit for a condition where pain is a daily reality, not an occasional event. Your parent's comfort and willingness to eat depend directly on how well their pain is controlled between meals and during them.
Don't settle for vague reassurances. The specifics matter.
The Cost of Senior Living With Chronic Pancreatitis
The national median cost for assisted living in 2025 is $6,200 per month, or $74,400 per year, according to the CareScout Cost of Care Survey. That's the base rate. For a resident with chronic pancreatitis, expect additional charges for specialized dietary preparation, enhanced medication management, and potentially a higher level of care assessment based on the complexity of daily needs. These add-ons can push monthly costs several hundred to over a thousand dollars higher depending on the community and your parent's specific care plan. At the higher end, you could be looking at $7,000 to $7,500 per month, which translates to $84,000 to $90,000 annually. Costs also vary dramatically by state, ranging from around $4,300 per month in Mississippi to over $9,000 in Massachusetts.
On top of room and board, pancreatic enzyme replacement medications are a significant ongoing expense. PERT is a lifelong requirement once exocrine insufficiency develops, and the medications aren't cheap. Financial assistance programs exist through manufacturers like AbbVie (Creon) and Allergan (Zenpep), though most are limited to patients under 65 who aren't on Medicare. For seniors on Medicare, coverage varies by plan, and copays can still be substantial. Factor enzyme costs into your total budget from the start, not as an afterthought. If your parent also needs home health visits, specialist copays, and nutritional supplements, the annual out-of-pocket costs beyond the base assisted living rate can add up quickly. Start tracking these expenses early so you aren't caught off guard.
How Families Can Support Better Daily Outcomes
Even after your parent moves into a senior living community, your involvement makes a difference. Keep a clear, written care plan that outlines enzyme dosing (specific lipase units per meal and per snack), dietary fat limits, pain management protocols, and emergency contacts for their gastroenterologist. Share this document with the community's nursing staff and dietary team, and update it after every specialist appointment.
Visit at mealtimes when you can. Not to check up on staff, but to stay connected with how your parent is actually doing. Are they eating? Are they gaining or at least maintaining weight? Are they taking enzymes consistently? These observations matter more than any monthly report. If you notice your parent losing weight again or complaining of increased pain after meals, that's information worth bringing to both the care team and the gastroenterologist promptly. Small changes caught early are far easier to address than a full nutritional crisis.
I've learned through my own caregiving experience that the best outcomes happen when families and care teams communicate openly. You know your parent better than anyone. The staff knows the daily routine. Together, you cover more ground than either can alone. That partnership doesn't end when your parent moves in. In many ways, it's just beginning.
Taking the Next Step With Confidence
Chronic pancreatitis is a condition that demands daily, structured attention to pain, nutrition, and enzyme management. It isn't something that gets easier to manage at home as your parent ages. The physical demands on caregivers are real, and the medical complexity of balancing pain relief with adequate nutrition requires consistent professional support that goes well beyond what most families can provide indefinitely.
If your parent has reached the point where eating has become a source of fear, where weight loss is accelerating despite your best efforts, or where the daily enzyme and dietary management has become more than your family can sustain, it's worth exploring senior living communities that specialize in complex medical needs. The right environment won't cure chronic pancreatitis. But it can give your parent the structured daily support that makes living with it more manageable. Your parent deserves to eat without dreading what comes next, and finding the right care environment is one of the most important things you can do to make that possible.