Your mother is sitting on the couch, leaning forward, palms flat on the cushion beside her hips. She pushes. Nothing happens. She shifts her weight, tries again, and sinks back into the same position. You watch her arms strain, her face tighten with effort, and you realize the problem isn't pain or stiffness. The muscles that should drive her body upward from a seated position simply aren't strong enough to do the job anymore.
This is what polymyositis looks like in daily life. It isn't dramatic or sudden. It's a quiet erosion of the proximal muscles, the large muscle groups closest to the center of the body: hips, thighs, shoulders, and upper arms. These are the muscles responsible for the movements most people never think about, like standing up from a chair, climbing a few stairs, or lifting your arms to wash your hair. When polymyositis weakens them, every surface your parent sits on and every environment they move through becomes either an ally or an obstacle.
For families watching this unfold, the question shifts quickly from "What is this condition?" to "How do we set up their world so they can still function?" That's where polymyositis senior living decisions get real. This article walks through what daily life actually looks like with this condition, why furniture height and environment design matter more than most families expect, and how to evaluate whether a senior living community can genuinely support someone with proximal weakness patterns that standard care models weren't designed for.
What Polymyositis Does to Daily Movement
Polymyositis is an autoimmune inflammatory myopathy, which means the body's immune system attacks its own muscle tissue, causing chronic inflammation and progressive weakness. Unlike conditions that affect the hands and feet first, polymyositis targets the proximal muscles symmetrically. Both hips weaken together. Both shoulders lose strength at roughly the same rate. The pattern is predictable, and that predictability is actually useful when planning care.
The weakness develops over weeks to months, not overnight. Your parent might first notice trouble climbing stairs or difficulty getting out of a low car seat. Over time, reaching overhead becomes harder. Washing hair, pulling a shirt on, retrieving something from a high shelf: these all require shoulder and upper arm strength that gradually fades. In some cases, swallowing and breathing muscles are also affected, though this varies widely between individuals.
Treatment typically involves corticosteroids like prednisone to reduce inflammation, often combined with immunosuppressive medications for long-term management. Many people respond well to treatment, but roughly 30% are left with some degree of permanent residual weakness even after the inflammation is controlled. That residual weakness is what shapes daily life and drives the need for environmental support.
The Daily Experience: What Families See at Home
The signs tend to accumulate quietly. Your parent stops using the downstairs bathroom because the toilet is too low. They avoid the living room sofa because they can't get out of it without help. They start eating standing at the kitchen counter because the dining chairs don't give them enough height to stand back up. These aren't random changes. They're adaptations to proximal weakness, and they tell you exactly which muscle groups are struggling.
Picture this: you take your parent to a restaurant, and they sit down in a standard dining chair without thinking about it. When the meal ends, they slide to the edge of the seat, press their hands down on the table, and try to push themselves upright. Their hip extensors and quadriceps, the muscles that power the stand-up motion, can't generate enough force. They try again. A waiter notices and offers an arm. Your parent looks embarrassed, but the real issue isn't embarrassment. Every chair, toilet, and bed in their environment needs to be at the right height, or they'll need hands-on help for something as basic as standing up.
I spent a decade helping people of all ages move through physical spaces safely, and one thing became clear early on: small design details make a bigger difference than most people realize. The height of a seat, the placement of a grab bar, whether a bed frame sits at 18 inches or 24 inches from the floor. These details are the difference between someone doing it themselves and someone needing to call for help every time.
Height Matters: How Furniture and Environment Design Support Polymyositis
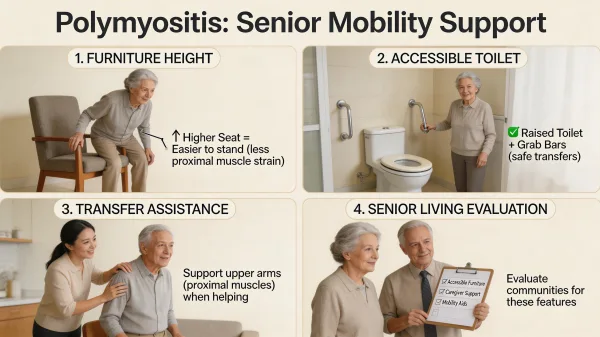
In practice, this is where things break down. A beautiful senior living community full of low sofas, deep armchairs, and standard-height toilets is functionally inaccessible for a polymyositis resident. The issue comes down to physics: standing up from a seated position requires the hip extensors and quadriceps to push the body's full weight upward against gravity. The lower the surface, the deeper the bend at the hip and knee, and the more muscle force required to complete the motion. For someone with proximal weakness, a seat height difference of just three or four inches can be the line between independence and needing physical assistance.
Standard residential toilets sit about 14 to 15 inches from floor to seat. For most older adults, that's already low. For someone with polymyositis, it's a trap. Comfort-height or ADA-compliant toilets raise that to 17 to 19 inches, which significantly reduces the muscular demand of standing. Raised toilet seats can add another 2 to 5 inches on top of existing fixtures, and when combined with grab bars mounted beside the toilet at the right height, they create a system that lets someone with moderate proximal weakness manage toileting independently. Research published in PMC found that adding grab bars to a standard-height toilet reduced the difficulty of the sit-to-stand motion for older women, and that combining a raised seat with grab bars changed muscle activation patterns in ways that reduced the overall physical demand of the task.
The same principle applies throughout the living space. Dining chairs should be firm, armless or with sturdy armrests, and high enough that the resident's hips are at or above knee level when seated. Deep cushioned sofas are the worst possible seating for someone with proximal weakness because they position the hips below the knees and create a longer, harder push to stand. Beds need to be at a height where the resident can sit on the edge with their feet flat on the floor and their thighs roughly parallel to the ground. Bed rails or assist handles mounted to the frame give something to push against when the hip muscles alone can't complete the motion.
Physical therapy plays a critical role alongside these environmental modifications, but the approach has to be specific. Standard "stay active" advice doesn't account for the inflammatory nature of polymyositis. Research from the Myositis Association and studies reviewed by PMC confirm that exercise is safe and beneficial for people with established polymyositis, including moderate-to-high intensity resistance training. But the program needs to be designed by a physical therapist who understands inflammatory myopathies. The goal isn't just general fitness. It's targeted strengthening of unaffected muscle groups, protecting muscles that are actively inflamed, and building enough functional capacity to perform daily transfers. Timing matters too: during an active flare, exercise intensity typically needs to drop, then ramp back up as inflammation comes under control. A good PT will focus on the exact movements that matter most: sit-to-stand transfers, stair negotiation, and safe reaching patterns. Pool-based exercise can also work well because water supports body weight while still allowing resistance training. Finding a therapist with myositis experience isn't always easy, but the Myositis Association maintains referral resources that can help.
When evaluating a senior living community for someone with polymyositis, ask specifically about furniture heights in common areas, toilet heights in resident rooms and shared bathrooms, bed frame options and whether assist devices can be mounted, and whether the community has a relationship with a physical therapist experienced in neuromuscular conditions. These aren't luxury features. For a polymyositis resident, they're the infrastructure that determines whether they can live there with any degree of independence or whether they'll need hands-on help for every transition throughout the day.
What to Look for in a Senior Living Community
Not every assisted living community is equipped to handle the specific needs of a polymyositis resident, and the differences aren't always visible on a brochure or a tour. The cosmetic quality of a community tells you very little about whether the physical environment will work for someone with proximal weakness. You need to look past the lobby and into the details.
During my time doing mobile X-ray work in care facilities, I saw beautiful buildings where residents couldn't get off the toilet without calling for help because nobody had thought about fixture heights. I also saw modest, older facilities where someone had clearly paid attention to how residents actually moved through their day. The difference wasn't about budget. It was about whether anyone had matched the environment to the residents' physical realities.
Start by sitting in the chairs in the dining room and common areas. Are they firm and upright, or low and cushioned? Ask about grab bar placement in bathrooms. Ask whether toilet heights meet ADA comfort-height standards. Find out whether the community can accommodate bed assist devices or adjust bed heights. Ask about staffing ratios and whether aides are trained in safe transfer techniques for residents with muscle weakness. A community that handles transfers well can prevent injuries to both residents and staff. A community that doesn't may rely on just pulling a resident up by the arms, which is uncomfortable and potentially dangerous.
Pay attention to the hallways and common paths between the dining room, activity spaces, and resident rooms. Long corridors without resting points can be exhausting for someone whose hip and thigh muscles fatigue quickly. Benches or chairs placed at intervals give your parent a place to pause without having to ask for help. Handrails on both sides of hallways matter too, not because your parent can't walk, but because having something to steady against reduces the muscular cost of covering distance.
Polymyositis Senior Living Costs and Care Levels
Assisted living costs vary significantly depending on location and the level of personal care needed. As of 2025, the national median cost of assisted living is approximately $6,200 per month, or about $74,400 per year, according to CareScout's Cost of Care Survey. Communities in the Northeast and West Coast tend to run higher, while parts of the Southeast and Midwest can be more affordable.
For a polymyositis resident, costs often land above the base rate. Most assisted living communities use tiered pricing or a la carte models, meaning you pay more as care needs increase. Transfer assistance, help with dressing (especially overhead garments), and mobility support throughout the day all add to the monthly bill. Families should expect to pay on the higher end of a community's range, and it's worth asking during tours exactly how additional care hours are billed. Some communities charge a flat rate per care tier, while others charge by the hour for each service. The difference can be hundreds of dollars per month.
When our family faced the financial side of long-term care, the gap between the quoted base rate and the actual monthly cost was one of the biggest surprises. Nobody tells you upfront how quickly the extras add up, and by the time you realize it, you're already committed.
The Role of Ongoing Medical Management
Polymyositis isn't a static condition. It flares and stabilizes, and the medication regimen requires regular monitoring. Corticosteroid use carries its own risks over time, including bone density loss, weight gain, high blood sugar, and a separate form of muscle weakness called steroid myopathy that can actually mimic the original disease. After nearly 20 years working in hospitals, I've seen how easily medication side effects get overlooked when the focus stays only on the primary diagnosis. Your parent's rheumatologist needs to stay in the loop, and the senior living community needs to support that relationship.
Ask whether the community coordinates transportation to specialist appointments. Find out if staff can recognize signs of a disease flare, like a sudden increase in difficulty with transfers or new trouble swallowing, and whether they know to report those changes to the care team promptly. A community that treats polymyositis as just "needs help getting up" is missing the clinical picture. The condition requires awareness that the level of assistance needed may change from month to month depending on disease activity and medication adjustments.
Helping Your Parent Adjust to Polymyositis Senior Living
The emotional weight of this transition is real. Your parent is dealing with a body that doesn't do what it used to, and moving into a community can feel like confirmation that things have gotten worse. That feeling is valid. Don't minimize it.
What helps is framing the move around function, not failure. A well-designed senior living environment doesn't mean your parent is less capable. It means the environment is finally working with their body instead of against it. When every chair is the right height and every bathroom has the right supports, your parent can focus on living their life instead of strategizing how to get through each physical transition. That shift can be freeing in ways neither of you expects.
Encourage your parent to stay involved in physical therapy after the move. The research consistently shows that exercise is safe and effective for people with polymyositis, including resistance training when supervised by a therapist familiar with inflammatory myopathies. Maintaining proximal strength, even at a reduced level, directly translates to more independence in daily tasks. That matters. A community with on-site or affiliated rehabilitation services makes it easier to keep therapy consistent, which is especially important during medication changes or after a flare when strength may have dropped.
Making the Decision
Choosing a senior living community for a parent with polymyositis comes down to a few clear questions. Can they get on and off the toilet without calling for help? Can they stand up from every chair in the common areas? Is the bed at the right height, and does it have assist options? Is there physical therapy available that understands this condition? Are the staff trained to help with transfers safely?
If the answer to most of those questions is yes, you've found a community that can work. If the answers are vague or the staff seems unfamiliar with proximal weakness patterns, keep looking. The right fit isn't about the nicest building. It's about the building that actually works for your parent's body.
You're doing the right thing by researching this carefully. Polymyositis is rare enough that most families have never heard of it before their parent's diagnosis, and finding a community that truly understands the condition takes effort. Having watched my own family scramble to evaluate care options while still processing a diagnosis, I know how overwhelming this phase feels. Trust what you see during tours, ask the specific questions that matter, and remember that the goal isn't perfection. It's finding a place where your parent can live as independently as their body allows, with the right support ready when they need it.