Non-Hodgkin Lymphoma and Senior Living: What Families Need to Know
Non-Hodgkin lymphoma (NHL) in a senior living context refers to the specific daily care challenges that arise when an older adult is undergoing active lymphoma treatment while living in an assisted living or similar care community. The focus isn't the cancer itself, but matching the predictable ups and downs of treatment to a care setting that can respond flexibly.
If your parent has been diagnosed with non-Hodgkin lymphoma and you're trying to figure out how to keep their daily life manageable while they go through treatment, you're probably exhausted. Between oncology appointments, blood draws, infusion days, and the side effects that follow, cancer treatment can feel like a full-time job for the whole family. And the hardest part is often what happens between appointments, when your parent is home and too wiped out to cook a meal or get out of bed safely.
I spent five years as a caregiver for my first husband during his cancer treatment, and one thing I learned early is that treatment doesn't just affect the days you're at the hospital. It reshapes every day in between. The exhaustion, the nausea, the brain fog, the sudden recovery that makes you think everything is fine until the next cycle hits. That rhythm becomes the backdrop for every decision you make about care.
This article covers what NHL treatment actually looks like on a week-by-week basis, why that pattern matters when choosing a senior living community, and what specific questions to ask so your parent gets the right level of help at the right time. The goal is practical: give you enough understanding of the treatment cycle to make a better housing decision.
How NHL Affects Older Adults Differently
Non-Hodgkin lymphoma is largely a disease of older adults. The median age at diagnosis is 67 to 68 years, and the incidence continues to rise in the elderly population. For seniors, NHL treatment carries additional weight because older bodies recover more slowly from chemotherapy, existing health conditions complicate treatment decisions, and the line between cancer-related fatigue and age-related decline can blur quickly.
Many older adults with NHL receive a regimen called R-CHOP, which combines three chemotherapy drugs, a targeted therapy drug called rituximab, and a steroid. Treatment typically runs six to eight cycles over 18 or more weeks. That's four to five months of active treatment where your parent's energy, immune function, and daily capabilities will swing dramatically from week to week. For families, this creates a care coordination problem that doesn't fit neatly into most senior living pricing models.
Comorbidities make things harder. Research shows that 87% of NHL patients over age 80 have at least one additional health condition at diagnosis, most commonly cardiovascular disease. Oncologists may use reduced-dose protocols for very elderly patients, sometimes called mini-CHOP, to limit toxicity. Even with reduced doses, the cyclical pattern of good weeks and bad weeks remains. From working in the ER, I've seen elderly patients come in with complications that weren't from their cancer at all, but from how the treatment interacted with conditions they already had. That layering effect is something families need to plan for, not react to.
The Chemo Cycle: What Predictable Fluctuation Means for Daily Care
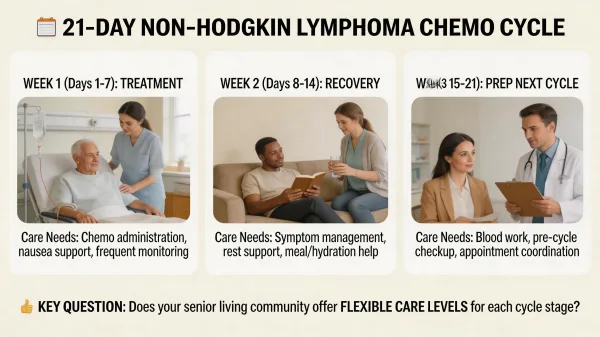
Understanding the R-CHOP cycle is the single most useful thing you can do when evaluating a senior living community for a parent with NHL. Each cycle runs 21 days, and the pattern repeats predictably. Day 1 is infusion day, when all the intravenous drugs are administered at the cancer center. Days 1 through 5 include oral steroids, which can cause restlessness, mood changes, and increased appetite. Then comes the waiting period, and this is where the real care challenges begin.
Between days 7 and 14, your parent's white blood cell count drops to its lowest point. This is called the nadir, and it's the most dangerous window in each cycle. During the nadir, your parent's immune system is at its weakest. A simple cold can become a medical emergency. Febrile neutropenia, a fever combined with critically low white blood cell counts, requires immediate hospitalization and intravenous antibiotics within the first hour. The body's primary defense against bacteria is functionally offline. Your parent may need to avoid communal dining, limit contact with sick residents, and have their temperature checked twice daily. Some oncologists prescribe growth factor injections like filgrastim to help white blood cells recover faster, but even with that support, the nadir period demands heightened vigilance. What makes this window especially tricky is that your parent may not look or feel sick during the early nadir days. The danger is internal, visible only in blood counts. By the time symptoms appear, the situation may already be urgent.
From my own experience as a spousal caregiver during cancer treatment, I can tell you that the nadir period is terrifying and invisible at the same time. My husband would look fine on the outside while his bloodwork told a completely different story. You learn to read the calendar like a weather forecast, knowing that days 8 through 12 are the days you cancel plans, watch for fevers, and keep the house as clean as a hospital room. Families going through this with a parent deserve a care community that understands this rhythm as well as they do.
The fatigue pattern follows a similar arc. Days 1 through 3 after infusion often bring the worst nausea and exhaustion. By day 5 or 6, the steroids wear off, and a deep fatigue sets in that can last through the nadir period. Around days 15 to 18, many patients start to feel noticeably better. Energy returns, appetite improves, and daily activities become manageable again. Then, around day 21, the next cycle starts and the pattern resets.
This is what makes NHL care so different from most senior living situations. Your parent doesn't need the same level of help every day. During the nadir and the post-infusion fatigue window, they may need full assistance with meals, bathing, medication management, and mobility. During the recovery window, they may only need light check-ins and companionship. A good care community structures its support around this cycle rather than locking your parent into a single, fixed care level for the entire month.
The Question No One Thinks to Ask
Here's the question that can save your family thousands of dollars and a lot of frustration: can this community adjust the level of care within the same month?
Most assisted living communities price their services in tiers. You pay a base rate for the room, and then a care level surcharge based on how much help your parent needs. The problem is that these tiers are typically set monthly and reviewed quarterly. If your parent is assessed during a bad week, they'll be placed at a high care level and billed accordingly, even during the weeks when they're feeling fine and don't need that help. If they're assessed during a good week, they might not get enough support during the nadir. I've watched families pay for round-the-clock care their loved one didn't need 60% of the time, simply because the billing structure couldn't flex with the treatment schedule.
Ask the community directly whether they can scale care up and down within the same billing period. Some communities offer what's called a "variable care" or "flex care" model. Others will work with you informally. The ones that can't, or won't, may not be the right fit for active cancer treatment.
Infection Control: What a Community Should Do
Immunocompromise is the biggest medical risk your parent faces in a communal living setting during NHL treatment. A senior living community housing a resident on chemotherapy needs protocols that go beyond standard practice. Look for communities that can isolate meals during nadir periods, either through in-room dining or separate seating. Staff should understand that a fever of 100.4 degrees or higher in your parent isn't a "wait and see" situation. It's a call to the oncologist and potentially a trip to the ER.
Ask about their illness notification policy. If another resident on the same floor has a respiratory infection, will you be told? Does the community have a relationship with a home health agency that can send a nurse for blood draws or growth factor injections on-site, or will your parent need transportation to a clinic every time? These aren't luxury features. During the nadir period, they're safety requirements.
What to Look for in a Senior Living Community During NHL Treatment
Beyond flexible care levels and infection control, there are practical features that make a community better suited for a parent going through lymphoma treatment. Transportation to and from the cancer center is a big one: infusion appointments can last several hours, and your parent will likely need a ride home. Nutritional support matters too, because chemotherapy often causes taste changes, mouth sores, and nausea that make standard dining menus unusable. A community with a kitchen willing to accommodate soft foods, bland options, or small frequent meals can make the difference between your parent eating enough and losing dangerous amounts of weight.
Look for staff who are trained in or at least familiar with oncology-related side effects. Peripheral neuropathy from vincristine, one of the R-CHOP drugs, can cause numbness and tingling in the hands and feet that increases fall risk. That's something a care team needs to know about and monitor.
Medication management is another area where communities vary widely. During active NHL treatment, your parent may be taking anti-nausea drugs, steroids on a specific five-day schedule, growth factor injections, antibiotics for infection prevention, and their regular daily medications. Getting that wrong isn't a minor mistake. Ask whether the community's medication management system can handle a medication list that changes from week to week based on where your parent is in the cycle. Some communities have on-site nurses who can coordinate directly with the oncology team. Others rely on third-party pharmacy services that may not be responsive enough for treatment that moves this fast.
Emotional support matters too. Chemotherapy is isolating, and the nadir period can force your parent into their room for days at a time. Communities that offer scheduled social check-ins, pastoral visits, or even simple companionship during low-energy days can make a real difference in how your parent copes with treatment. Cancer treatment is hard on the body, but the loneliness of it can be just as damaging.
Understanding the Costs of Senior Living During Cancer Treatment
The financial side of NHL treatment combined with senior living costs adds up quickly. As of the 2025 CareScout Cost of Care Survey, the national median cost for assisted living is $6,200 per month, or $74,400 per year. That's the base rate before any care level surcharges, which can add $1,000 to $3,000 or more per month depending on the level of assistance your parent needs.
If your parent requires a higher care tier during treatment, you could be looking at $8,000 to $10,000 per month during active chemotherapy, dropping back to the base rate once treatment ends. Over a six-cycle R-CHOP course lasting about five months, that's roughly $40,000 to $50,000 in senior living costs alone, not counting oncology bills, medications, or supplemental home health services. The financial shock of cancer care on top of senior living costs catches most families off guard. I watched my own family scramble to piece together costs when a loved one needed memory care, and cancer treatment adds another expensive layer to an already overwhelming equation. Talk with a hospital social worker or financial counselor early in the treatment process. Many cancer centers have staff dedicated to helping families understand insurance coverage, out-of-pocket maximums, and state programs that may offset some of the cost burden. Waiting until the bills arrive to figure out a plan makes a hard situation harder.
Making the Right Decision for Your Family
Choosing a senior living community for a parent with non-Hodgkin lymphoma isn't like choosing one for general aging support. The treatment cycle creates a care pattern that most communities aren't designed for, and it's your job to find the ones that can adapt. Start by talking with your parent's oncology team about the expected treatment timeline, the specific drugs being used, and the anticipated side effects. Bring that information to every community tour. Ask the oncology nurse to write down the expected nadir window and the typical side effect timeline so you can share it with potential communities in plain terms.
Ask the tough questions about flexible billing, infection protocols, and staff training. Don't settle for a community that treats your parent's cancer treatment as an afterthought. The right community won't just house your parent during treatment. It will become part of the care team, adjusting support as the cycle demands and keeping your parent safe during the most vulnerable windows.
You're making this decision during one of the hardest stretches your family will face. Give yourself credit for doing the research, and trust that the effort you put into finding the right community now will pay off in fewer emergencies, less burnout, and better quality of life for your parent through treatment and beyond.