Your mother walks into the living room she's lived in for thirty years, everything in its familiar place, the couch and coffee table exactly where they've always been. She moves confidently, looking straight ahead, until her hip collides hard with the corner of the table she has walked past a thousand times. She stops, confused, and checks herself, not distracted and not rushing, just completely certain she didn't see it. That moment, quiet and a little embarrassing and easy to dismiss, is how most families first run into the reality of advanced glaucoma.
Your parent isn't clumsy, and they aren't losing their mind. Their visual field has narrowed so far that anything outside a shrinking central cone has gone invisible to them, even objects they've lived beside for decades. This article looks at what glaucoma vision loss senior families actually see and don't see, why home environments quietly become dangerous, and how to tell when glaucoma senior living placement is the safer choice. It covers the paradox that trips so many families up, the daily demands of the disease, what to look for in a community built for low vision, and the costs you'll weigh along the way.
I've cared for people across the entire spectrum of ability, from infants in my own daycare to patients in their nineties on an ER table, and one thing that transfers across all of them is the ability to sense when someone's spatial awareness has slipped out of sync with what they still seem able to do. Glaucoma produces exactly that mismatch, which is part of what makes it so easy for everyone around the patient, including the patient, to miss the problem until something goes wrong.
Understanding Glaucoma and the Vision You Lose First
Glaucoma is a group of eye diseases that damage the optic nerve, usually from pressure building inside the eye. It's the leading cause of irreversible blindness worldwide, and in the United States, about 4.22 million adults live with it, roughly 2.56% of people over 40. After age 60, the risk climbs sharply, and Black adults are affected at more than twice the rate of White adults.
What makes glaucoma different from other eye diseases is what it takes first. Cataracts fog up the whole picture, and macular degeneration blurs out the center, but glaucoma attacks the edges. Peripheral vision loss senior readers may not even notice for years, because central vision, the part you use to read a menu or recognize your daughter's face, often stays sharp until the disease is far along. Research estimates that up to 40% of optic nerve fibers can be damaged before a person realizes anything is wrong, which is why the condition is often called the silent thief of sight.
Tunnel Vision: What Your Parent Actually Sees and Why It's Dangerous
Glaucoma doesn't take vision evenly. It eats the outer edges of the visual field and works inward. Early on, that shows up as small blind patches in the upper or nasal periphery, the kind a person can live with for years without noticing. The brain is remarkably good at filling in those gaps. It pulls from memory, from expected patterns, from the other eye, and from context. Your parent's brain stops waiting to actually see the floor in their kitchen and simply assumes the floor is there, because it has always been there. That compensation works until it doesn't.
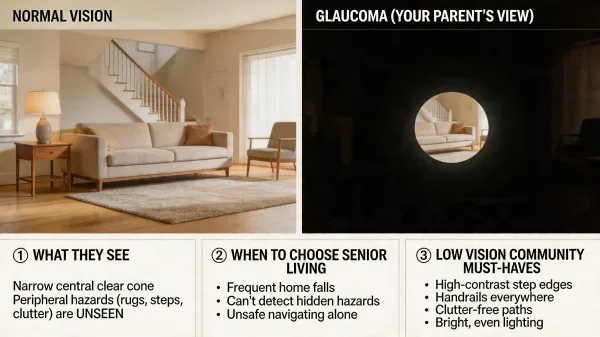
As the disease progresses into the moderate and advanced stages, those blind patches fuse into larger defects. The visual field narrows from all sides inward, leaving a shrinking cone of central clarity, and this is what's meant by tunnel vision. Your parent still sees what they look directly at, often in crisp detail, but everything outside that cone is gone, not blurry, not dim, just absent. A coffee table in the blind zone doesn't register as fuzzy or dark, it registers as nothing at all, and the brain has no way of knowing it's missing.
That's why glaucoma falls look different from other senior falls. An older adult with arthritis or weakness typically trips on an uneven surface or a rug edge, while an older adult with advanced glaucoma walks directly into objects. Research has linked advanced glaucoma to roughly eight times the fall risk of age-matched peers without the disease, with inferior visual field damage especially tied to stumbles and fear of falling. The hazards are the ones that sit to the side at hip or knee height and don't extend into the narrow forward cone: chair arms, open drawers, pet bowls, the corner of a counter, a walker someone left by the door. Anything that would normally catch the eye in peripheral vision is invisible.
Caring for young children teaches you to read spatial awareness almost before you read anything else. A toddler who can name every animal in a book but keeps walking into the edge of the dining table is telling you something about their visual processing, not their intelligence. Years of running a daycare, and then years of wheeling portable X-ray equipment into care facilities where I watched residents move through hallways, drilled that same pattern recognition into me from the other end of life. When I see a sharp, capable older adult who still reads the newspaper and recognizes every grandchild but clips their shoulder on the same doorframe twice in ten minutes, I'm not thinking about confusion or dementia, I'm thinking about visual field. Glaucoma is the condition most likely to produce that exact mismatch.
Most families don't realize how much their parent has lost until something breaks, often a hip or a wrist or the back of a head. The tunnel vision fall risk isn't theoretical, and it isn't a small bump on a probability curve. It's a fundamental change in how your parent moves through space, and the home they've lived in for decades is actually the most dangerous place for it, because every object in that home was placed and arranged for someone with normal peripheral vision. A fifteen-year-old coffee table, a hallway runner, the cat's water bowl, the corner of the kitchen island, all of it was invisible-to-normal-vision before, and now a fair portion of it is invisible to your parent.
Where This Gets Confusing: The Paradox of Preserved Central Vision
Here's the part that trips families up. Your parent can still read, still recognize your face from across a room, still watch television and play a card game and sometimes even thread a needle on a good day. So when you ask them, "Can you see okay?" they say yes, and they aren't lying. Their central vision, the part glaucoma attacks last, is working.
But a person can have excellent central acuity and still have almost no usable peripheral vision. The eye chart at the doctor's office tests the center. It doesn't tell you whether your father can see the stair banister two feet to his right or the grandchild toddling up on his left. Families often discover this only after a fall, when the hospital discharge paperwork mentions visual field loss that nobody had framed as a safety issue before. I've watched adult children sit in waiting rooms visibly shocked that "20/30 vision" and "dangerous blindness on every side" were both true of the same parent.
The Daily Reality of Advanced Glaucoma
Once glaucoma reaches the advanced stage, it stops being a checkup item and starts shaping every hour of the day. Glaucoma daily living breaks down across a few specific demands that overlap and compound each other.
Glaucoma Eye Drop Management
Most glaucoma is managed with prescription eye drops that lower pressure inside the eye, taken once or twice a day, every day, for life. Missing doses lets pressure climb and accelerates further nerve damage. Research on chronic-disease adherence finds that patients typically take 30 to 70% of prescribed doses, and roughly half discontinue within the first few months. For eye drops specifically, up to a quarter of patients miss doses simply because they can't get a drop into the eye. Hand tremors, arthritis, poor fine-motor coordination, and the peripheral vision loss itself all make a one-inch target genuinely hard to hit. Someone has to notice when the bottle isn't going down as fast as it should.
Mobility and Navigation
Getting from the bedroom to the bathroom at 2 a.m. is the kind of routine that kills people with advanced glaucoma. Low light collapses the residual vision further, and unfamiliar objects, say a laundry basket someone left in the hallway, sit squarely in the blind zone. Stairs are worst of all, because depth perception depends on both eyes sweeping the edge of each step, and glaucoma damages that edge detection first. Many seniors with advanced glaucoma stop using stairs entirely, even when they're still physically capable of climbing them.
Recognizing When Home Care Isn't Enough
Not every glaucoma patient needs senior living. Early and moderate glaucoma, well-controlled with drops and regular ophthalmology visits, is compatible with living independently for years, sometimes decades. The decision to move usually arrives when the disease crosses into advanced territory and the home environment stops being neutral.
A few signals tend to land around the same time. Your parent has had one or more falls in the past year, especially the kind where they walked into something they should have seen. They've stopped going into certain rooms, or stopped using stairs, or stopped leaving the house after dark. Medications are being missed, or doubled, because they can't see the labels or the drops aren't going in. Meals are being skipped because reading the stove dial or the microwave has become hard. The house is staged the way it was staged when they were sighted, and nobody can realistically rearrange an entire home around tunnel vision and keep it that way.
When several of those signals show up together, advanced glaucoma assisted living is worth looking at seriously. The purpose of the move isn't to remove your parent's independence. It's to place them in an environment that was designed, staffed, and lit for what they can still see, with fewer variables that their visual field can't catch.
What to Look for in a Senior Living Community for Glaucoma
Senior living communities vary enormously in how well they accommodate low vision, and marketing brochures don't tell you much about the real day-to-day experience. Walk through a community yourself, preferably at more than one time of day, and pay attention to what a tunnel-vision resident would actually encounter at hip height, at knee height, and off to the sides where their vision can no longer catch things.
Lighting That Actually Helps
The Illuminating Engineering Society publishes lighting standards specifically for older adults and the visually impaired (ANSI/IES RP-28), and the short version is that seniors with low vision need roughly two to three times the light level a younger adult would find comfortable, delivered without glare or harsh shadows. In a good community, hallways are evenly lit with no dark stretches between fixtures, stairwells are brightly lit from top to bottom, and bathrooms have night lighting on motion sensors. Watch for glare off polished floors and windows, which can wipe out the residual vision a glaucoma resident still has.
Contrast and Layout Consistency
Glaucoma adaptive living depends heavily on visual contrast. Doorframes that contrast with walls, light switches that stand out from the surface behind them, plate edges that differ from tablecloths, handrails in a color that reads against the corridor, all of these give residual peripheral vision something to catch. Ask whether the community uses consistent color cues for wayfinding. Ask whether furniture in common areas stays in the same place month after month, because a resident with tunnel vision memorizes layouts and any change becomes a fall waiting to happen.
Staff Awareness of Low Vision
This is where facility visits during my mobile X-ray years taught me the most. I'd walk into a lovely-looking lobby and then find residents navigating hallways where staff had parked cleaning carts in the middle of the corridor because "the residents know to go around." Residents with glaucoma don't go around. They walk into the cart. Ask the staff specifically how they handle residents with visual field loss. Ask whether aides are trained to approach a low-vision resident from the front, announce themselves, and describe what they're doing. Ask how the community manages eye drop schedules and whether nursing staff, not the resident, administers glaucoma medications for residents who can't reliably self-dose. A community that has real answers to those questions is a different place than one that gives you a brochure and a rate sheet.
The Cost of Senior Living When Glaucoma Drives the Decision
The financial picture for glaucoma-driven placement tracks the broader senior living market, and it isn't cheap. As of 2025, the national median monthly cost of an assisted living community was $6,200, which works out to $74,400 a year, according to the CareScout Cost of Care Survey. That's a median, meaning roughly half of communities cost more. In coastal and metropolitan markets, $8,000 to $10,000 per month is common.
If your parent's care needs progress past what assisted living can handle, nursing home rates in 2025 ran a national median of $315 per day for a semi-private room, or about $114,975 a year, and $355 per day for a private room, roughly $129,575 annually. In-home care as an alternative runs about $35 per hour, which comes to roughly $80,080 a year at 44 hours a week, and climbs quickly if your parent needs overnight supervision.
Medicare doesn't cover room and board in assisted living or long-term nursing home care. It pays only for limited skilled nursing after a qualifying hospital stay. Medicaid covers long-term nursing home care for those who qualify financially, and many states offer Home and Community-Based Services waivers that can help with assisted living, but eligibility and benefits vary widely by state. Long-term care insurance, VA benefits for eligible veterans, and private funds round out the usual payment sources. Most families end up blending several. Starting that conversation before a crisis makes the math less brutal.
Helping Your Parent Make the Transition
The move itself is harder for a glaucoma patient than for a fully sighted resident, because your parent has been relying on memorized layouts to function. Dropping them into an unfamiliar apartment means every object is in a blind zone, and you should expect a rough two to four weeks of adjustment. Help them walk the unit and the common areas in the same pattern every day until the new layout lives in memory. Place furniture with low-vision principles in mind from the first day, and don't rearrange afterward. Label drawers and shelves in large, high-contrast print, and work with the community to get eye drop administration set up before move-in day rather than after. Most families find that once the environment stabilizes, their parent's mobility and confidence rebound more quickly than expected, because the community was built for them in a way the old house never could be.
Bringing It All Together
Advanced glaucoma narrows your parent's world to a forward-facing cone while leaving their central vision clear enough to hide how much they've lost. That mismatch is what makes the disease so easy to underestimate and so dangerous in a home environment designed for normal peripheral vision. The fall risk isn't abstract, the eye drop regimen isn't optional, and the quiet withdrawal from stairs, dim rooms, and nighttime routines is usually the disease talking, not fatigue.
Senior living isn't a defeat. For the right family, at the right point in the disease, it's a practical match between what your parent can still see and what their environment demands of them. Take the time to visit communities in person, ask the questions that actually matter for low vision, and work through the numbers before a fall forces the timeline. Your parent has spent decades building the life they have. The next chapter can be safer without being smaller. Start the conversation while they can still be part of it.