Research shows that 15 to 30 percent of adults diagnosed with dermatomyositis also have an associated cancer, with the risk climbing sharply for those diagnosed after age 50. That statistic alone makes dermatomyositis more than a muscle condition. It's a diagnosis that demands immediate and thorough medical attention, and it's one that most families haven't heard of until it shows up in their parent's medical chart.
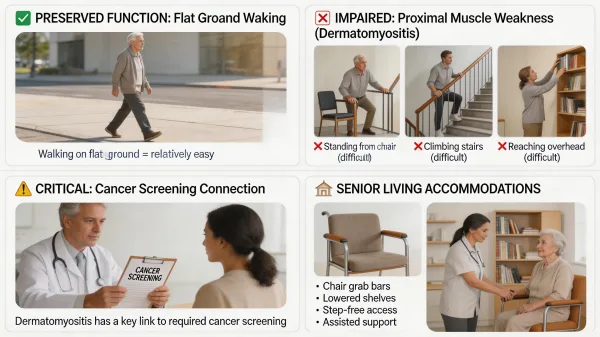
Dermatomyositis is a rare inflammatory myopathy that causes progressive proximal muscle weakness and a distinctive skin rash, affecting roughly 1 in 100,000 adults per year. For seniors, this condition makes everyday tasks like standing from a chair, climbing stairs, and reaching overhead increasingly difficult, while walking on flat surfaces often remains surprisingly intact.
That selective weakness pattern catches most families off guard. Your parent might walk across the living room without trouble but can't get up from the couch without pulling on furniture. They can stroll down a hallway and carry on a conversation, but they can't lift their arms high enough to wash their own hair. The gap between what they can do and what they can't doesn't make sense until you understand which specific muscles dermatomyositis attacks.
Having spent nearly two decades working with patients in hospital settings, I've seen how these proximal weakness patterns tell a very specific diagnostic story. A patient who walks fine on flat ground but can't manage a single stair step is showing you exactly which muscle groups are failing, and it's that clinical pattern recognition that helps families understand why their parent needs targeted support rather than general assistance.
If your parent has been diagnosed with dermatomyositis and is losing the ability to handle basic daily tasks, senior living may enter the conversation earlier than you expected. This article breaks down how dermatomyositis affects daily function, why cancer screening at diagnosis is critical, what treatment looks like on a practical level, and what to look for in a dermatomyositis-friendly senior living community.
The Proximal Weakness Pattern: Why Some Tasks Are Impossible While Others Are Fine
Dermatomyositis targets proximal muscles, the large muscle groups closest to the center of your body. These include the muscles of the hips, thighs, shoulders, upper arms, and neck. The distal muscles in the hands, feet, lower legs, and forearms are typically spared until much later in the disease, if they're affected at all. This creates a selective weakness pattern that looks confusing from the outside but follows a very specific logic.
Consider a parent who can walk across a room at a normal pace but can't stand up from a dining chair without using both arms to push off the armrests. Or a mother who manages her morning walk around the block but needs help getting out of bed because the hip flexors and thigh muscles required to sit up and swing her legs over the side have weakened significantly. Walking on flat ground is largely a momentum-driven activity that relies on different muscle engagement than standing up, climbing, or reaching overhead. The muscles that propel you forward aren't the same muscles that lift your body weight against gravity.
Getting up from chairs, toilets, and beds requires the quadriceps and hip flexors to lift the full weight of the body from a low, seated position. Climbing stairs demands that thigh and hip muscles raise body weight upward with each step. Reaching overhead to shampoo hair, grab items from upper cabinets, or even pull on a shirt depends on shoulder and upper arm strength that deteriorates early in the disease. Neck flexor weakness can make it difficult to lift the head from a pillow, affecting how your parent gets out of bed each morning. All of these movements share one thing in common: they require the proximal muscles to work hard against gravity, and those are the exact muscles dermatomyositis breaks down.
I've worked with patients in the hospital whose weakness fit this exact profile. They'd walk to the radiology department from their room without difficulty, then couldn't climb onto the X-ray table without significant assistance. You could see the frustration on their faces because the weakness didn't match their own sense of what they could do. That disconnect is the hallmark of proximal muscle weakness, and it's the reason dermatomyositis requires such specific environmental modifications in any living situation.
For senior living, this pattern dictates very specific environmental needs. Your parent requires single-floor living or reliable elevator access with zero stairs in their daily routine. Raised toilet seats and grab bars become essential equipment, not optional upgrades. Shower chairs and handheld showerheads address the inability to raise arms overhead for extended periods. Chairs throughout the living space need firm, higher seats with armrests that allow pushing up rather than pulling. Beds may need to be adjustable or fitted with assist rails. And because dermatomyositis in adults carries a six-fold increased risk of malignancy compared to the general population (with the highest risk in the first two years after diagnosis), every new diagnosis should trigger comprehensive cancer screening.
The Cancer Screening Question No One Thinks to Ask
Here's what too many families aren't told at diagnosis: dermatomyositis in adults, especially those over 50, is strongly linked to underlying cancer. The overall cancer rate in dermatomyositis patients ranges from 9 to 32 percent depending on the study, and patients between the ages of 50 and 69 face the steepest risk. The most commonly associated cancers include ovarian, lung, breast, colorectal, and pancreatic types. In many cases, the dermatomyositis is actually the body's immune response to a hidden malignancy, meaning the muscle and skin symptoms can serve as a warning sign that cancer is present but hasn't been detected yet.
This risk peaks within the first one to three years after dermatomyositis diagnosis. Comprehensive screening should include age-appropriate and gender-appropriate tests (mammography, colonoscopy, pelvic exams, chest imaging), along with thorough blood work and imaging of the chest, abdomen, and pelvis. Your parent's rheumatologist should be coordinating this screening, but if it hasn't been discussed, bring it up yourself and make sure you get clear answers about what's been done and what still needs to happen.
When my own family member received a serious diagnosis, I learned quickly that you can't assume every doctor is communicating every critical detail to the family. In the chaos of a new diagnosis, information falls through the cracks, and families are often too overwhelmed to know which questions they should be asking. I've carried that lesson into how I think about patient care ever since. The cancer screening question for dermatomyositis isn't something most families know to raise on their own, and if the treating physician doesn't bring it up proactively, it can go unaddressed during the window when screening matters most. Be the person who asks the uncomfortable question. Your parent's care team should welcome it, and if they don't, that tells you something too.
How Dermatomyositis Is Treated and What That Means for Senior Living
There's no cure for dermatomyositis, but treatment can slow progression and improve muscle strength over time. The first-line treatment is typically high-dose corticosteroids (usually prednisone) to reduce muscle inflammation quickly. Because long-term steroid use carries its own serious side effects, including bone loss, weight gain, diabetes risk, and increased vulnerability to infections, doctors usually add immunosuppressant medications like methotrexate or azathioprine as steroid-sparing agents. For patients who don't respond to standard treatment, intravenous immunoglobulin (IVIg) therapy has shown effectiveness in improving both muscle strength and skin symptoms, though it requires regular infusion visits that can take several hours each session.
What this means for your parent's daily life is a schedule that revolves around medication timing, regular blood work, specialist appointments with their rheumatologist and potentially a dermatologist, and careful monitoring for both disease flares and medication side effects. Physical therapy plays a critical role in maintaining whatever muscle strength remains and should begin once active inflammation is under control. The goal isn't just to preserve function but to rebuild strength in muscles that have already been damaged by inflammation.
Any senior living community your parent moves into needs to accommodate frequent medical appointments, coordinate multiple medications (some of which may require infusion visits at an outside clinic), and understand that your parent's functional abilities may fluctuate significantly from week to week as treatment is adjusted. A community that expects stable, predictable care needs won't be the right fit for dermatomyositis.
What a Dermatomyositis-Friendly Senior Living Community Looks Like
Not every assisted living community is equipped to handle the specific demands of dermatomyositis. The condition requires a combination of physical accessibility, medical coordination, and staff awareness that goes beyond standard senior care. Physical layout matters most. Your parent's unit should be entirely on one level with no steps between rooms, and the bathroom should be fitted with a walk-in shower (no tub to climb over), a raised toilet, grab bars, and a shower seat. Common areas need to be accessible without stairs, and seating throughout should be firm and high enough for someone with proximal weakness to stand from without major effort.
Staff need to understand the fluctuating nature of this condition. Your parent might manage well independently on a good day and need significant help on a bad one. This isn't a condition with a steady, predictable decline. Flares happen, medication changes affect strength levels, and the care plan needs flexibility built into it. Staff should know that helping someone stand up from a toilet or a chair isn't the same as helping someone who can't walk at all. The assistance your parent needs is targeted and specific, focused on the movements where proximal weakness creates the barrier rather than on general mobility support.
During my years doing mobile X-ray work inside care facilities, I saw how much difference it made when staff understood a resident's specific limitations versus treating every resident with the same general approach. Residents whose staff knew their condition received better, faster, more dignified help. A community that takes the time to learn the proximal weakness pattern will provide far better daily care than one that applies a generic assistance protocol to everyone.
Skin Sensitivity and Sun Exposure in Dermatomyositis Senior Living
The skin component of dermatomyositis creates its own set of challenges in a senior living environment. The characteristic rash (a purplish discoloration around the eyes, across the chest, on the knuckles, and along the shoulders) is photosensitive, meaning sun exposure can trigger or worsen flares. Your parent's community needs to offer shaded outdoor areas and understand that sun avoidance is a medical requirement, not a personal preference.
Activities that involve prolonged outdoor time (gardening programs, walking groups, outdoor dining) need to be managed carefully with appropriate sun protection measures in place. Sunscreen, protective clothing, and awareness from activity staff all matter. Skin care routines may also include prescription topical treatments that require proper storage and consistent application, so medication management should account for these alongside the oral and infusion medications being used for the muscle component of the disease.
Choosing the Right Community: Questions That Matter
When evaluating senior living options for a parent with dermatomyositis, the standard tour questions won't cover everything you need to know. Walk the actual unit your parent would live in and check for step-free access, bathroom equipment, and furniture height. Sit in the chairs they'd use daily and see how easy they are to stand from. These details matter more than how the lobby looks.
Ask whether the community has experience with residents who have inflammatory myopathies or autoimmune conditions requiring immunosuppressant medications. Find out how they handle fluctuating care needs and whether their care plan can adjust week to week without requiring a formal reassessment each time. Ask about transportation to specialist appointments (rheumatology, dermatology, oncology) and whether staff can coordinate multiple prescription schedules, including any infusion therapies that happen off-site.
As of 2025, the national median cost for assisted living is approximately $5,900 to $6,200 per month, which works out to roughly $70,800 to $74,400 annually. Higher-acuity care with additional medical coordination can push that figure upward, and communities with more hands-on medical support tend to charge at the higher end of the range. For a condition like dermatomyositis that requires ongoing specialist involvement and flexible daily care, budgeting for the higher end is realistic.
Supporting Your Parent Through a Rare Diagnosis
Dermatomyositis is a rare condition, and that rarity can make the search for the right senior living community feel isolating. Most communities won't have specific experience with this particular diagnosis, but what matters is that the physical environment matches your parent's functional needs, the staff understands conditions that fluctuate, and the medical coordination is strong enough to keep up with ongoing treatment demands.
Having watched families face unexpected diagnoses that changed everything about their care plans, I know how disorienting this process feels. The condition itself is manageable with the right treatment, and the right living environment can make a real difference in your parent's quality of life and your own peace of mind. Focus on the specifics: single-floor access, proper bathroom equipment, flexible care plans, and a team that listens when you explain what your parent needs. Those aren't extras, they're the foundation of good care for this condition.
Your parent's diagnosis doesn't define what their life looks like from here. With the right support in place, they can maintain comfort, dignity, and daily routines that work around the condition rather than being controlled by it.