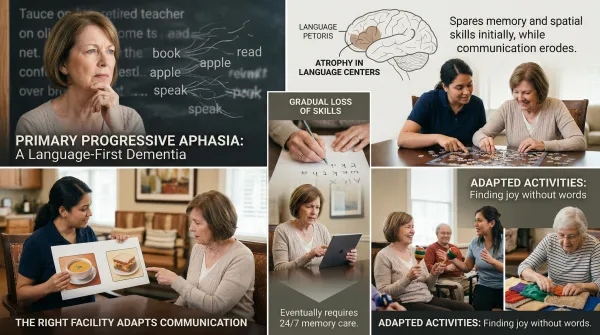
Primary progressive aphasia (PPA) is a neurodegenerative condition that gradually destroys a person's ability to speak, understand language, read, or write, while memory and other cognitive functions often remain intact for years. Unlike Alzheimer's disease, where memory loss comes first, PPA targets the brain's language network. Over time, though, it progresses into broader dementia, and primary progressive aphasia memory care becomes the most appropriate level of support.
If your parent's memory seems fine but they're struggling to find words, follow conversations, or read a book they used to love, you're probably asking a confusing question: is memory care even the right option for someone whose memory still works? The answer, for most families dealing with PPA, is yes. But the path there looks different than it does for Alzheimer's, and the facility you choose needs to understand that difference.
Imagine your mother was always the storyteller in the family, the one who read to the grandkids, the one who could hold a dinner table captive with a funny story from her week. Then you start noticing pauses mid-sentence. She substitutes odd words, calling a fork a "stick" or referring to the dog by the wrong name. She stops initiating phone calls. Her children assume she's depressed or withdrawing socially. It can take months, sometimes longer, before anyone considers that this isn't a mood problem. It's a language problem. And it's progressing.
That's the reality of PPA, and this article explains what it looks like, why memory care eventually becomes the right fit, and what adapted care should include for someone whose thinking is intact but whose words are disappearing.
What Primary Progressive Aphasia Looks Like in a Parent
PPA comes in three recognized variants, each attacking language in a different way. The nonfluent/agrammatic variant causes halting, effortful speech and broken grammar. Your parent might drop small words from sentences or speak in a telegraphic style, saying "go dinner Mom" instead of a full sentence. The semantic variant strips away word meaning. Your parent can still speak fluently, but they lose comprehension of individual words and may not recognize common objects by name. The logopenic variant, which is most closely linked to Alzheimer's pathology, causes frequent word-finding pauses and difficulty repeating phrases back.
Symptoms typically appear between ages 50 and 70, and PPA is classified as a rare disease, affecting roughly 3 per 100,000 people. What makes it so disorienting for families is that the person can still recognize loved ones, manage daily routines, and think clearly for years after diagnosis. The problem is isolated to language. I've worked with patients in the hospital who could follow every instruction I gave them through a gesture or a nod but couldn't tell me where it hurt. That gap between what someone understands and what they can express is one of the hardest things for families to wrap their heads around.
Early signs are easy to misread. A parent who stops calling on the phone, who goes quiet at family dinners, or who suddenly seems uninterested in reading might look like someone dealing with depression. The distinction matters because PPA requires a completely different care approach than a mood disorder, and the earlier your parent's doctor evaluates for language-based neurodegeneration, the more time your family has to plan.
Why Primary Progressive Aphasia Eventually Requires Memory Care
PPA is a dementia. That's the part many families don't hear clearly at first. The word "aphasia" sounds like a speech problem, not a brain disease. But PPA is caused by the same types of neurodegeneration that cause frontotemporal dementia and, in some cases, Alzheimer's disease. Language goes first, but it doesn't stop there.
Over a span of roughly 7 to 10 years from symptom onset, most people with PPA develop impairments in memory, judgment, behavior, or daily functioning that extend well beyond language. But the language loss itself creates safety risks long before those broader changes arrive. A person who can't call 911 in an emergency, can't explain their symptoms to a doctor, or can't understand medication instructions needs supervised care. Consider a parent who takes multiple prescriptions daily. If they can no longer read the labels or comprehend a pharmacist's spoken instructions, medication errors become a real and dangerous possibility. That's where memory care fits. It isn't just about memory in the literal sense. It's about providing 24-hour support for people whose cognitive decline, whatever form it takes, makes independent living unsafe. The name "memory care" describes the structure of the care, not a single symptom it treats.
I've seen families wait too long because the label didn't match. Their parent could still do laundry, still remember birthdays, still find their way around the neighborhood. But they couldn't ask for help if something went wrong. That's a safety gap, and memory care is designed to close it.
Families often assume that PPA and memory care are a mismatch, but the reality is more practical than the terminology suggests. Memory care communities are staffed around the clock, designed for people who need cognitive support, and structured to prevent the kind of crises that arise when someone can't communicate their own needs. That description fits PPA.
How Memory Care Adapts for Language-Based Dementia
This is the section that matters most, because not every memory care facility is equipped to support a resident with PPA. Standard memory care programming is built around verbal interaction. Staff give spoken reminders. Activities involve group conversation, trivia, storytelling, or singing along to familiar songs. For a resident with Alzheimer's who can still speak but has memory gaps, that works. For a resident with PPA who can't produce or process spoken language, it's a daily source of frustration and isolation.
Facilities that understand language loss dementia use visual communication systems throughout the building. Picture-based schedules posted in the resident's room show what happens next: meals, activities, rest time. Communication boards with icons for common needs (pain, bathroom, hungry, tired) give residents a way to express themselves without words. Some facilities use tablet-based communication apps that let the resident tap images or pre-recorded phrases. These tools aren't extras. For a PPA resident, they're the difference between participating in daily life and sitting silently while the world talks around them.
Staff training is the other half of the equation. Caregivers working with PPA residents need specific coaching on reading nonverbal cues: body language, facial expressions, gestures, and behavioral signals that communicate what words can't. This kind of attentiveness isn't something most people are born with. It's built through practice. I spent years in my parents' daycare and then ran my own for a decade, caring for young children who couldn't yet tell me what they needed. You learn to read posture, eye contact, restlessness, the way someone pulls away from food versus the way they push a plate aside when they're full. You notice when someone is holding their body stiffly because they're in pain, versus when they're just tired and want to sit down. That same instinct is exactly what care staff need when working with PPA patients. The person still has thoughts, preferences, and emotions. They still know when they're being rushed or ignored. The language is gone, but the person is not.
Speech-language pathologists (SLPs) play a critical role in PPA and memory care that many families don't know to ask about. An SLP working within a memory care setting can train staff on communication techniques specific to each resident's variant of PPA, introduce compensatory strategies as language declines, and help families adjust how they interact during visits. Some SLPs also work with residents on script training, practicing short, rehearsed phrases for daily situations to preserve functional speech as long as possible. Research from the speech therapy field shows that strategies put in place early, before language loss becomes severe, are far more effective than those introduced after the person has already lost most verbal ability.
Activity programming needs to shift too. Art, music (listening and rhythm-based, not lyric-dependent), gardening, and movement activities keep residents engaged without requiring verbal participation. I remember caring for a toddler in my daycare who barely spoke a word for the first six months but would light up during music time, clapping along and smiling at the other kids. Connection doesn't require conversation. A good memory care program meets the person where their abilities are, not where a standard checklist says they should be.
Questions to Ask a Memory Care Facility About Language Loss
Here's the question no one thinks to ask when touring a memory care facility: how does your staff communicate with residents who can't speak?
Most families evaluate a facility by talking to the staff, reading brochures, and watching how caregivers interact with residents during a visit. But if your parent has PPA, the question isn't whether the staff are friendly and articulate. It's whether they know what to do when a resident can't respond verbally. Ask whether the facility has experience with PPA or other language-based dementias specifically. Ask whether staff receive training on nonverbal communication techniques. Ask whether they use visual schedules, communication boards, or assistive technology. Ask whether a speech-language pathologist is involved in care planning. If the answers are vague or the staff seem unfamiliar with PPA, that's valuable information.
Your parent needs a team that understands aphasia dementia care as its own category, not a variation of Alzheimer's they'll figure out along the way. Having spent nearly 20 years working inside hospitals, I can tell you that the facilities that do this well are the ones that talk about specific systems, not just general compassion. Compassion matters, but systems are what keep your parent from being overlooked when they can't speak up for themselves.
After a PPA Diagnosis: Where to Start
A PPA diagnosis changes the timeline and the playbook, but it doesn't erase your parent's identity or your ability to support them well. The progression is real and it's hard, especially for families who are watching someone lose the very thing that connected them: conversation, stories, the sound of their voice saying your name.
Start by connecting with a speech-language pathologist early, even while your parent is still living at home. The strategies they put in place now will carry forward into memory care later. Consider voice banking too, which lets your parent record their own voice saying common words and phrases for use on a communication device down the road. When the time comes to evaluate facilities, prioritize the ones that can show you, not just tell you, how they support residents with language loss. And if you're feeling overwhelmed by a diagnosis that doesn't fit neatly into the boxes you expected, know that you're not the first family to stand in this confusing spot. The right care exists. It just takes knowing what to look for.